Neurological System
Common Assessment and Diagnostic Test:
Computed tomography (CT)
- Detects hemorrhage, infarction, abscesses and tumors
- Informed consent when contrast dye is required
- Can be with or without injection of contrast dye
- Assess for Allergic reaction to contrast dye or shellfish prior to administration
- Note that some clients may be given the dye even if they report an allergy; they may be
treated with an antihistamine and corticosteroids before the injection to reduce the severity - Inform the client that there may be a hot, flushed sensation and a metallic taste in the mouth when the dye is injected.
- Encourage PO fluids
Note: Assess the need to withhold metformin if iodinated contrast dye is used for a diagnostic procedure because of the risk for metformin-induced lactic acidosis.
Lumbar puncture
Preprocedure:
- Explain procedure
- Informed consent
- Lateral recumbent position at edge of bed
Postprocedure:
- Neuro assessment every 15-30 minutes until stable
- Position flat for several hours(1hr)
- increase oral fluid intake and monitor I&Os
- monitor vital signs
- Check CSF leakage
- Administer analgesics for spinal headache as prescribed
Cerebral Angiography
Identifies aneurysms, vascular malformations, narrowed vessels
Preprocedure:
- Informed consent
- Assess allergies, renal function, and anticoagulation therapy
- Lie flat; dye injection into femoral artery via catheter
- Adequate hydration
- Neuro assessment; mark peripheral pulses
- Pre-procedure sedation
- Inform the client that there may be a hot, flushed sensation and a metallic taste in the mouth when the dye is injected.
Postprocedure:
- Monitoring: VS, Neurological assessment 15-30 min till stable, puncture site Q1hr
- Immobilize affected extremity 6-8 hours
- Keep flat in bed for 12-14 hours post procedure
- Assess distal pulses and check for CMS
- Encourage fluid intake
- Assess for allergic reaction
Electroencephalography
Records electrical activity in the brain
Preprocedure:
- Kept awake night before (to induce sleep)
- Withhold stimulants or sedative drugs (24 - 48h pre procedure)
- Allow for oral intake of nutrition as normal
- Completed by technician via bedside
Post-procedure:
- Seizure precaution
- Maintain safety
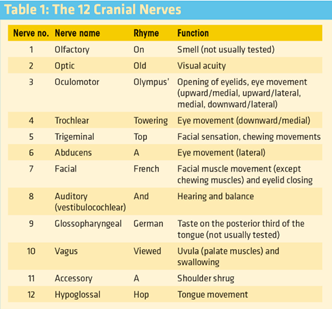
Cranial Nerves
Cranial nerve examination: https://www.registerednursern.com/cranial-nerve-examination-nursing/
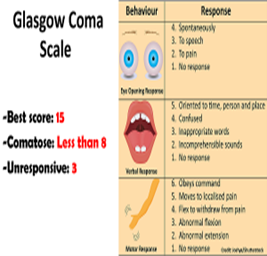
Glasgow Coma Scale (GCS)
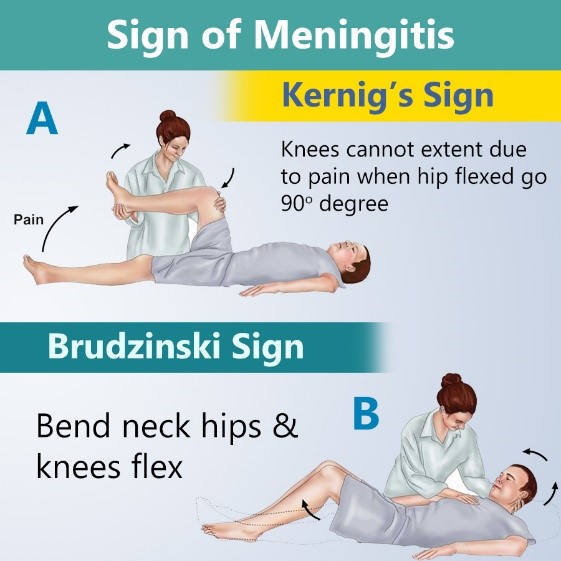
Meningitis
Signs of Meningeal Irritation
- Irritability/ change in LOC
- Nuchal rigidity
- Severe, unrelenting headaches
- Generalized muscle aches and pains
- Nausea and vomiting
- Headache and fever
- Photophobia
- Abnormal pupil reaction and eye movement
- Kernig’s Sign: inability to straighten the leg completely when it is fully flexed at the knee and hip
- Brudzinski’s Sign: involuntary flexion of the hip and knee when the neck is passively flexed
Causes: Infection (viral, bacteria and fungal)
Implementation:
- IV ABX therapy
- Monitor vital signs and lab values
- Droplet precautions
- Vaccine prevention
Increased Intracranial Pressure
- Normal: 5 – 15 mmHg (>20 mmHg…needs treatment)
- Early signs: Mental status change or Altered LOC
- Late signs: Vital sign changes (increased BP, decreased pulse rate)
What can cause increased pressure within the skull that leads to increased intracranial pressure?
- Head trauma
- increased in cerebrospinal fluid
- hemorrhage
- hematoma (subdural and epidural)
- hydrocephalus: buildup of CSF in the brain
- tumor: putting pressure on brain
- encephalitis (inflammation of brain tissue) or meningitis (inflammation of membrane covering spinal cord and brain)
Signs and Symptoms:
- Mental Status Changes- (Early sign)
- Irregular breathing (Cheyne-stokes breathing)
- Nerve changes- pupillary changes (Early sign)
- Decerebrate or decorticate posturing
- Decorticate (flexor posturing)

- Decerebrate: (Extension posturing)

- Cushing’s Triad: (Late sign) herniation of the brain stem
- Seizures
- Vital sign changes: Increased systolic blood pressure (widening pulse pressure), decreased heart rate, and abnormal breathing
Nursing Interventions:
- Monitor Vital signs, pupillary reactions, GCS, and muscle strength
- Position head of bed: 30 to 45 degrees, proper alignment of head (midline)
- NO flexion of neck or hips
- Straining activities AVOIDED: vomiting, coughing, sneezing, Valsalva, agitation (keep environment calm), avoiding restraints as necessary
- Prevent Valsalva maneuver
- Maintain respiratory function limit suctioning to as needed
- Monitor temperature- prevent shivering (increases metabolic needs= increased ICP)
- Monitor ventriculostomy (external ventricular drain): monitors ICP. It’s a catheter inserted in the lateral ventricle to assess ICP and drains CSF during increased pressure readings.
- Administer osmotic diuretics, corticosteroid therapy, and antiseizure medications as prescribed
CVA/Stroke
Type of Strokes
–Ischemic (most common): due to a blood clot within a blood vessel or stenosis of an artery that feeds the brain tissue. This limits the blood that can reach the brain cells. This type of stroke can happen due to:
- Embolism: where a clot has left a part of the body (example the heart: this can happen due to a heart valve problem or atrial fibrillation). The clot develops in the heart and travels to the brain, which stops blood flow.
- Thrombosis: Clot forms within the artery wall within the neck or brain. This is seen in patients with hyperlipidemia or atherosclerosis
–Hemorrhagic: this occurs when there is bleeding in the brain due to a break in a blood vessel. Therefore, no blood will perfuse to the brain cells. In addition, this can lead to excessive swelling from the leakage of blood in the brain. Causes of this type of stroke includes: rupture of a brain aneurysm, uncontrolled hypertension, or aging blood vessels (older age).
-TIA (transient ischemic attack) also called a mini-stroke. This is where signs and symptoms of a stroke occur but last only a few minutes to hours and resolves. It is a warning signs an impending stroke may occur. If this occurs the patient needs to seek treatment.
Risk Factors for stroke:
“Strokes Happen”
Smoking
Thinners (blood)
Rhythm changes (a-fib/flutter)
Oral Contraceptive
Kin (family history)
Excessive weight
Senior citizens
Hypertension
Atherosclerosis
Physical inactivity
Previous TIA
Elevated blood lipids/ blood sugar (diabetes)
ANeurysm
Signs and Symptoms of a Stroke:
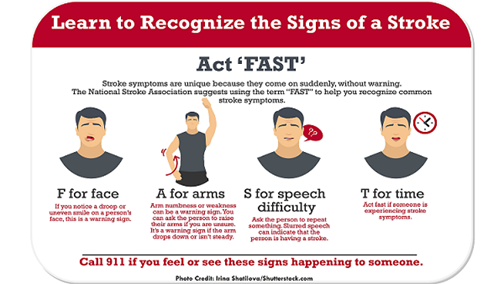
“FAST”
Face: drooping or uneven smile
Arm: numbness, weakness, drift (raise both arms)
Speech: can’t repeat a phrase, slurred speech
Time: to call rapid response and note the time
**National Stroke Association recommends using the mnemonic F.A.S.T. to help assess for signs and symptoms quickly.
Other assessment data:
Bowel and bladder incontinence
Aphasia: unable to speak (comprehending or producing it)
- Receptive Aphasia: unable to comprehend speech (Wernicke’s area)
- Expressive Aphasia: comprehends speech but can’t respond back with the correct words, if at all (Broca’s area)
- Mixed Aphasia: combination of the two types of aphasia.
- Global Aphasia: complete inability to understand speech or produce it.
Dysphagia: issues swallowing (weak muscles)
Hemianopia: limited vision in half of the visual field
Hemiparesis: weakness on one side of the body
Diagnosis
- CT scan
- MRI
Nursing interventions:
- Administer TPA (thrombolytic) within 3 hours from symptom onset
- Monitor for bleeding with TPA administration
- Prevent Increased ICP
- Maintain ABCs
- Position Q2hr/ proper body alignment
- Active and passive range of motion
- Monitor bowel and bladder elimination
- Address communication needs- face client, speak clearly and slowly, use verbal and nonverbal communication
- Do not approach visually impaired side
- Assist with feeding- facilitate swallowing through proper positioning, place foods on unaffected side of mouth, use tongue, encourage semisolid foods, maintain upright positioning after eating
- Assess for neglect syndrome- ignoring the affected side
Spinal Cord Injury
- Can lead to loss of motor function, sensation, reflex activity, and bowel and bladder control
- Complications: respiratory failure, autonomic dysreflexia, spinal shock, further cord damage, and death.
- Common: Cervical—C5, C6, and C7, Thoracic—T12, Lumbar—L1
Assessment:
- Respiratory status changes
- Sensory and motor paralysis below the level of injury
- Low of reflexes
- Loss of bladder and bowel control
- Presence of sweat (not on paralyzed areas)
- Tetraplegia (Quadriplegia: between C1 and C8
- Paraplegia: between T1 and L4
a. Cervical injuries
- C2 to C3 – fatal
- C4 – major innervation to the diaphragm
- C5 to C8 – may move shoulder, decrease respiratory reserve
b. Thoracic level injuries
- Loss of movement of the chest, trunk, bowel, bladder, and legs may occur
- Leg paralysis (paraplegia) may occur
- Autonomic Dysreflexia - injuries above T6
c. Lumbar and Sacral Level
- Absent motor and sensory of lower extremities
- S2 to S3: neurogenic bladder
- Above S2 injury – unable to ejaculate.
- S2 to S4 – X erection and ejaculation.
Emergency Management
- Assess respiratory pattern/maintain airway
- Prevent head flexion, rotation or extension
- Maintain body in extended position
- Log roll the patient
- No part of body to be twisted or turned
- Not allowed to sit
- Cervical fracture – in the ED placed immediately in skeletal traction.
Interventions: Respiratory Care
- Assess respiratory status: C4 injuries (intercostal and abdominal muscle paralysis)
- Monitor ABG and maintain mechanical ventilation
- Deep breathing and incentive spirometer
- Signs of infection: Pneumonia
Interventions: Cardiovascular Care
- Monitor for cardiac dysrhythmias
- Assess bleeding and hemorrhage
- Assess for signs of shock
- Assess lower extremities for deep vein thrombosis (DVT)
- Measure circumference of calf and thigh
- Apply antiembolism stockings, assess for skin integrity
- Monitor orthostatic hypotension
Interventions: Neurological system
- Assess neuro status, motor and sensory
- Monitor for Autonomic Dysreflexia
- Immobilize the client
- Assess pain, initiate measures
- Monitor complication of immobility
- Prep for surgery
- Collaborate with physical therapy (PT) and occupational therapy (OT)
Interventions: Gastrointestinal system
- Assess distention and hemorrhage
- Monitor bowel sounds and paralytic ileus
- Prevent bowel retention
- Bowel control program
- Adequate nutrition and high fiber diet
Spinal shock
- Temporary loss of motor, sensory, reflex, and autonomic function (immediate)
- lasts less than 48 hours.. continues for several weeks
Assessment:
- Flaccid paralysis
- Loss of reflex activity below injury
- Bradycardia
- Paralytic ileus
- Hypotension
Neurogenic shock
- Injuries above T6 (soon after)
- Massive vasodilation occurs
Assessment:
- Hypotension
- Bradycardia
Autonomic Dysreflexia
- also known as autonomic hyperreflexia
- occurs after the period of spinal shock is resolved,
- injuries above T6 and cervical
- caused by visceral distention
Priority Interventions:
- Raise the head of the bed.
- Loosen tight clothing
- Check for bladder distention or other noxious stimulus.
- Administer an antihypertensive medication.
- Document.
Assessment:
- Sudden onset, severe throbbing headache
- Severe hypertension
- Flushing above the level of the injury
- Pale extremities below the level of the injury
- Nasal stuffiness
- Nausea
- Dilated pupils or blurred vision
Parkinson's Disease
- Loss of Dopamine, more acetylcholine leading to overstimulation (tremors, rigidity, bradykinesia)
- Occurs at older age (60+)
- signs and symptoms are subtle, maybe present to one side of extremity
- No cure
Motor symptoms:
- Tremors at rest (most common): hands, arms, legs, lips and tongue, “pill rolling”
- Stiffness of extremities (akinesia)… “freeze up”
- Shuffling of gait
- Cogwheel rigidity
- Bradykinesia
- stooping, depression, constipation, loss of smell
Alzheimer's Disease
SIGNS AND SYMPTOMS
The helpful thing about these terms, since we are talking about Alzheimer’s disease (which starts with the letter A), is that all these terms start with the letter A and end with ia:
Apraxia: inability to perform a certain motor activity (ex: can’t perform the movements to use a toothbrush or fork)
Aphasia: can’t understand speech or create speech to communicate
Agnosia: can’t recognize everyday objects, people, or interpret their senses (taste, sound, smell etc.)
Amnesia: memory loss (starts with short and them progresses to long term)
Anomia: inability to recall the name of objects…may make up words to call the object
Nursing Interventions & Treatment for Alzheimer’s Disease
7 M’s
Memory: often reorient patient, remind patient and show how to use objects they have forgotten how to use, keep tasks simple, don’t belittle the patient for forgetting
Movement: help keep the patient as independent as the disease allows because this helps with motor skills and body strength: maintain routines, incorporate exercises, easy fun games and things that are easy they like to do
Mental Health: keep calm during outbursts and use calm voice, provide with distractions. Give time to respond, don’t hurry patient, be aware of Sundowner’s in some patients and prepare (encourage a calm relaxing environment)
Maintain Safety: poor judgement (no driving, cooking alone or using dangerous objects).
Watch for wandering (patient loses the ability to recognize places and people along with keeping time) can become lost very easily
Interventions for Wandering:
WANDER
Wear a medical identification bracelet or GPS tracking device (disguised as a watch or placed in the shoe)
Avoid stressful, unfamiliar places (crowds, loud areas this can confuse and stress the patient which causes wander)
Needs met: bathroom, food, and liquid needs
Display signs that provide cues to the patient: label the rooms of the house on their doors and place reminders or warning signs
Exercise important: needs an organized day that has periods of activities they enjoy (create a safe place for the patient to wander and walk) and rest
Remove assess to doors or windows by keeping them locked with alarms and obscure the locks and alarms, hide keys to car
Communication Interventions
PATIENT
Pick one question or instruction step to give at a time (repeating may be necessary)
Avoid correcting or arguing (intense tones or anger facial expression can cause stress)
Take time for patient to speak and respond
Identify yourself directly in front of patient rather than behind (patient may react in a fearful or impulsive way)
Eye contact on eye level rather than standing is important (feels less intimidating to the patient)
Nonverbal communication helpful especially in late stage: act out, point, or use images
Talk in a normal tone that is clear and slow (not loud and fast), eliminate outside noises
Seizures
Occur when abnormal electrical signals are being rapidly fired for neurons in the brain.
Causes: Head injury, stroke, CNS infection, fever, brain tumor, drug withdrawal, epilepsy
1. Generalized: seizure is affecting both parts of the brain
a. Tonic-clonic (formerly called grand -mal):
- May experience AURA (warning a seizure is about to happen)
- Loses consciousness (at risk for injury)
- Will experience a tonic phase: body stiffens, breathing stops followed by cyanosis)
- Then a clonic phase: recurrent jerking of extremities (patient may have incontinence of stool or/and urine)
- Usually lasts no more than 3 minutes
- Status epilepticus- seizure activity greater than 5 minutes is an emergency
- If greater than 5 minutes or having multiple seizures in a row…activate emergency response team
- Post ictus (duration: hours to days): this is the recovery period: patient will feel very tired, extremely sore from muscle stiffening and jerking, can’t remember what happened
b. Atonic (drop attacks):
- Patient loses muscle tone
- Maintain patient safety
c. Myoclonic:
- Brief jerking extremities
2. Focal
a. Simple focal- motor seizure where the patient remains conscious and reports an aura
b. Complex focal- Client blacks out for a few seconds and experiences Automatisms: this is where they are performing an action without knowing they are doing it like lip smacking, rubbing hands together, or grasping for something that isn’t there
3. Non-motor seizures:
a. Absence Seizure (formerly called petit-mal)
- Most common in pediatric patients
- Daydreaming brief LOC
- Unaware, blank stare with movements
Interventions:
Seizure Precautions:
- At bedside have suction and oxygen ready
- IV access (to given anti-seizure medication, if needed)
- padded siderails
- pillow under head (to protect head)
- bed in the lowest position
- remove objects that can cause injury
2. What to do when your patient has a seizure?
- Protect patient if they are standing-up or sitting down by:
- gently lying the patient down and turning them onto their side.
- DO NOT restrain patient or try to hold the patient down
- Protect their head and extremities (pillow and bed pads will help with this)
- DO NOT put anything in the patient’s mouth
- Remove anything that can impede breathing or break
After seizure:
- Position patient on their side to prevent aspiration
- Provide o2 and suction as needed
- Reorient the patient
- Descriptive documentation of the event (identify triggers, onset, length of time, type of movements, areas involved, automations, loss of consciousness, post seizure)
Prevention of seizures:
- Avoid triggers (alcohol, stress, caffeine, fever, hyperventilation)
- Ketogenic diet (high fat, low carb)
- Adequate medication regimen
Bell’s Palsy

Interventions:
- Facial exercises, face sling
- Protect eyes (dryness and injury)
- Oral care, chew on unaffected side
ALS (Amyotrophic Lateral Sclerosis)
- Progressive, degenerative disease involving the lower motor neurons of the spinal cord and cerebral cortex; voluntary motor system involvement leads to a mixture of spastic and atrophic change in cranial and spinal musculature
Assessment:
- Aspiration precaution
- Tongue fatigue
- Facial fasciculations
- Progressive muscle wasting, atrophy, spasticity
- Dysarthria
- Respiratory insufficiency (resulting in death)
- No alteration in autonomic, sensory, or mental function
Interventions:
- Care is directed toward the treatment of symptoms.
- Monitor respiratory status and institute measures to prevent aspiration.
- Prepare to initiate respiratory support.
- Assess for complications of immobility.
- Address advance directives as appropriate.
- Provide the client and family with psychosocial support.
Guillain-Barré syndrome
An autoimmune neuro condition where the immune system attacks the nerves in the peripheral nervous system and cranial nerves
Causes:
- Recent upper respiratory illness or gastrointestinal infection (especially Campylobacter jejuni)
- Vaccine (swine flu etc.)
- Surgery
- Epstein-Barr virus HIV/AIDS, flu infection
Course:
- Acute, rapid ascending sensory and motor deficit that may stop at any level of CNS
- Protracted, develops slowly
- Prolonged course with phases of deterioration and remission
Assessment
- Paresthesia
- Motor loss usually beginning in lower extremities and working up towards the trunk
- Inadequate autonomic dysfunction- hypotension, tachycardia, vasomotor flushing, paralytic ileus, excess sweating
Nursing Interventions
- Symptom management
- Administer as prescribed (corticosteroids, plasmapheresis, IV immunoglobins, adrenocorticotropic hormone)
- Maintain patent airway (suctioning, raise HOB, mechanical ventilation)
- Aspiration precaution
- Maintain safety during mobility
- Active and passive ROM
- Maintain adequate nutrition and hydration
- Bowel and bladder regimen
- Manage pain
Multiple sclerosis
Chronic and progressive demyelination of white matter in brain and spinal cord that leads to paraplegia and paralysis
Assessment:
- Early- Vision, motor sensation changes
- Late- Cognitive and bowel changes
- Muscular incoordination
- Ataxia
- Tremors
- Nystagmus (diplopia)
- Dysphagia
- Impaired speech
Nursing Interventions for Multiple Sclerosis
- PT/ OT therapy
- Encourage adequate hydration and nutritional intake
- Administer meds as prescribed: immunosuppressants, corticosteroids, antispasmodics, monoclonal antibodies
- Bladder and bowel training
- Eye patch for diplopia
- Emotional support
Myasthenia Gravis
An autoimmune condition where the body attacks the receptors that allow for voluntary muscle control, which leads to muscle weakness. (No loss of sensation or atrophy occurs)
Signs and symptoms
- Diplopia
- Impaired speech
- Dysphagia
- Ptosis
- Fatigue
- Respiratory distress
Nursing interventions:
- Administer meds as prescribed (anticholinergics, corticosteroids, immunosuppressants)
- Eye care
- Active and Passive ROM
- Avoid factors that may cause myasthenia crisis (infection, stress, etc)
- Monitor for myasthenia crisis: sudden inability to swallow, speak or maintain airway






