The structures and functions of bowel elimination are associated with the ingestion of food and elimination of the waste products of digestion in the form of feces. Many factors can affect a person’s bowel elimination, including developmental level, emotional and cultural factors, dietary and fluid intake, activity, medications, perioperative issues, and physiological problems. Nurses
must understand the basic anatomy and physiology of the gastrointestinal system and the issues that impact a client’s bowel elimination to better meet clients’ nursing needs.
A. Structures of the gastrointestinal (GI) system
1. Mouth
- Includes lips, cheeks, hard and soft palates, gums, tongue, tonsils, and salivary glands.
- Structures move in concert to chew food (mastication), mix food with saliva to form a rounded mass of food (bolus), and move the bolus toward the posterior pharynx where it is swallowed.
2. Esophagus.
- Collapsible muscular tube that extends from the posterior pharynx, through an opening in the diaphragm, to the stomach.
- Secretes mucus and facilitates movement of food from the mouth to the stomach.
3. Stomach.
- Elongated C-shaped pouch mainly in the epigastric area of the abdomen. The cardiac sphincter is at the connection between the esophagus and the upper portion of the stomach; the pyloric sphincter is at the connection between the duodenum and the lower portion of the stomach.
- Stores and liquefies food.
- Secretes gastric juices (e.g., gastrin, pepsin, hydrochloric acid, intrinsic factor, and mucin).
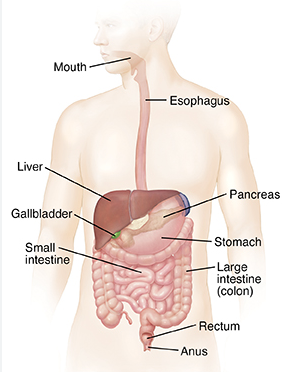
4. Small intestine.
- Tubular structure approximately 1 inch in diameter and 28 feet long that progresses from the duodenum, to the jejunum, to the ileum.
- Involved with digestion and absorption of nutrients.
- Secretes the enzymes sucrose, lactase, and maltase.
- Secretes cholecystokinin, which stimulates the gallbladder to release bile. e. Receives secretions from the liver, gallbladder, and pancreas.
5. Large intestine.
- Tubular structure approximately 2.5 inches in diameter and 5.5 feet long that progresses from the cecum, to the ascending colon, transverse colon, descending colon, sigmoid colon, rectum, and anus.
- Absorbs water and sodium ions and temporarily stores feces.
- Produces mixing movements and wave-like movements (peristalsis)that create a fecal mass, move waste product toward the anus, and promote defecation.
6. Vermiform appendix.
- Blind-end small tubular structure at the cecum beyond the ileocecal valve.
- Part of the immune system.
7. Liver.
- Large structure located in the upper right quadrant of the abdomen that consists of thousands of lobules that drain bile through the hepatic duct.
- Involved in protein, carbohydrate, and fat metabolism; secretes bile, which emulsifies fats, acts as a vehicle for excretion of bile pigments and cholesterol, and facilitates the absorption of the fat-soluble vitamins A, D, E, and K.
8. Gallbladder.
- Small sac that lies underneath the liver; the cystic duct exits the gallbladder and connects with the hepatic duct; the cystic and hepatic ducts unite and form the common bile duct, which drains bile through the sphincter of Oddi into the duodenum.
- Concentrates and stores bile.
9. Pancreas.
- Comma-shaped structure that extends from the duodenal curve to the spleen in the epigastric and upper left areas of the abdomen.
- Secretes the enzymes trypsin, lipase, and amylase, which are transported to the duodenum via the pancreatic duct.
- Contains islets of Langerhans.
- Alpha cells secrete the hormone glucagon, which promotes an increase in the amount of blood glucose.
- Beta cells secrete insulin, which decreases blood glucose and facilitates the metabolism of carbohydrates, proteins, and fats.
B. Functions of the GI system
1. Digestion.
- Mechanical digestion: Changes the consistency of food by mastication and mixing it with saliva and moves it through the GI system by swallowing and peristalsis.
- Chemical digestion: Splits compounds into small segments (e.g., hydroxyl group into one fragment and the hydrogen atom into another) in preparation for absorption and metabolism (hydrolysis).
2. Absorption.
- Small molecules as a result of chemical decomposition of a compound by the addition of water (hydrolysis)move against a concentration gradient (active transport)through the intestinal mucosa into the circulatory system.
- Most nutrients are absorbed in the small intestine; most water is absorbed in the large intestine.
3. Metabolism.
- Includes all the chemical reactions involved in energy production and expenditure.
- Anabolism is the synthesis of larger compounds from smaller compounds.
- Catabolism is the breakdown of complex compounds into simple compounds releasing energy for further body processes (e.g., muscle contraction, heat production).
- b. Metabolism requires energy.
- Carbohydrates are the preferred source of fuel for energy; cells catabolize glucose first, sparing proteins and fats; most cells catabolize fats next, sparing protein.
- Excess glucose is converted to glycogen and stored in the liver (glycogenesis).
- The liver converts protein or fat into glucose (gluconeogenesis).
- When blood glucose decreases, gluconeogenesis increases and glycogen from the liver breaks down releasing glucose (glycogenolysis).
C. Factors affecting bowel elimination
1. Developmental level.
- Toddlers: Develop intestinal control at about 2 to 3 years of age.
- Pregnant women: Enlarged uterus imposes on intestinal structures, resulting in decreased peristalsis.
- Older adults: Experience decreased peristalsis.
2. Emotional and cultural factors.
- Lack of privacy: Some cultures are open and others prefer privacy when attending to bodily functions.
- Inadequate amount of time to defecate.
- Embarrassment: Fecal elimination is often associated with sights and odors that may be offensive to others and make the client self-conscious.
3. Nutrition.
- Lack of fiber and excessive milk: Results in a decrease in peristalsis.
- Irregular eating patterns: Can interfere with regularity of bowel movements or decrease peristalsis.
- Caffeine and fiber promote peristalsis.
4. Fluid intake.
- Need 6 to 8 glasses of water daily.
- Decreased fluid intake causes constipation.
5. Activity.
- Activity increases muscle tone and stimulates peristalsis.
- Inactivity contributes to decreased muscle tone and constipation.
6. Medications.
- Antibiotics destroy normal intestinal flora.
- Antacids often slow peristalsis.
- Iron causes constipation.
- Analgesics, opioids, and antimotility drugs slow peristalsis.
- Laxatives and cathartics increase peristalsis.
7. Perioperative issues: Anesthesia and handling of the bowel during surgery may slow motility and cause cessation of peristalsis (adynamic ileus, postoperative ileus, paralytic ileus).
8. Physiological problems: Common problems include GI infections, food allergies, cancer, diverticulosis and diverticulitis, irritable bowel syndrome, and malabsorption syndromes.
II. Nursing Assessment of Bowel Elimination
The first step of the nursing process is assessment. When collecting information relative to a client’s GI status, the nurse obtains a client history, performs a physical assessment and assesses the characteristics of stool. This section provides guidelines to facilitate a comprehensive assessment of a client’s gastrointestinal status.
A. Obtain a health history regarding bowel habits and patterns
- Previous bowel habits and patterns and any changes.
- Dietary habits, use of supplements, change in appetite, and daily fluid intake.
- Level of activity, mobility, and exercise.
- Presence of pain or discomfort.
- Past and present illnesses, injury, and surgery that might affect GI function.
- Use of medications that can affect GI function, such as antibiotics, iron, laxatives, cathartics, antacids, and analgesics.
- Ability to self-toilet.
- Emotional status and current stressors.
- Social history (e.g., number of people using one bathroom, cultural background).
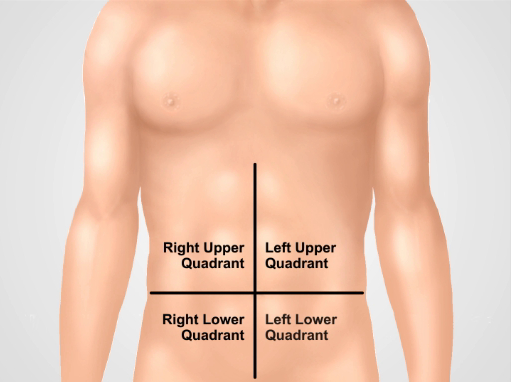
B. Physical assessment related to bowel elimination
1. Follow a systematic pattern when assessing the abdomen; four abdominal quadrants.
2. Assess color and integrity of the abdomen via inspection.
- Normal findings.
- Uniform color.
- Unblemished; silverfish white stretch marks (striae); possible surgical scars.
- Deviations.
- Tense, glistening skin, possibly indicating edema, ascites, or flatulence.
- Purple striae, possibly indicating rapid weight loss or gain or Cushing’s syndrome; rashes; other lesions.
3. Assess contour of the abdomen via inspection.
- Normal findings: Flat; round (convex); scaphoid (concave).
- Deviations.
- Abdominal distension.
- Requires a further focused assessment.
- Measure the abdominal girth with a centimeter tape measure around the body at the level of the umbilicus to obtain base line measurement.
- Assess for ascites by placing the hands on each side of the abdomen while pushing against the abdomen with one hand and feeling for the presence of fluid exerting pressure against the other side of the abdomen (fluid wave test).
- Assess for hypoactive bowel sounds via auscultation.
4. Assess symmetry of the abdomen via inspection.
- Instruct client to take a deep breath.
- Normal findings: Symmetrical appearance.
- Deviations.
- Enlarged liver and spleen become more prominent.
- Localized protrusions may indicate an umbilical or inguinal hernia or a tumor.
5. Assess for presence of vascular patterns on abdomen.
- Normal findings: No visible prominent veins.
- Deviations: Dilated veins visible, particularly around umbilicus (caput medusa); associated with ascites, liver disease, and portal hypertension.
6. Auscultate the abdomen for bowel sounds.
- Disconnect nasogastric tube suction if present.
- Follow a logical sequence.
- Listen in each area for 1 minute.
- Normal findings.
- High-pitched, irregular musical sounds or gurgles (borborygmi).
- Occur every 5 to 15 seconds and last 1 to several seconds.
- Deviations.
- Hyperactive: Loud, frequent sounds occurring about every 2 to 3 seconds; caused by increased peristalsis associated with diarrhea, gastroenteritis, and early bowel obstruction.
- Hypoactive: Soft, infrequent sounds occurring about one per minute; caused by decreased intestinal peristalsis associated with anesthesia, abdominal surgery, or conditions such as bowel infections, obstruction, or impaired innervation.
- Absent: No sounds heard after listening for 5 minutes.
7. Auscultate the abdomen for vascular sounds.
8. Percuss the abdomen to determine position, size, and/or density of underlying structures.
- Percuss several areas in each quadrant of the abdomen using a systematic sequence.
- Normal findings.
- Tympany over the stomach and gas-filled intestine.
- Dullness over the liver, spleen, and full bladder; no tenderness.
- Deviations.
- High-pitched tympany heard with distention.
- Large dull areas associated with organ enlargement, tumors, and presence of fluid.
9. Palpate the abdomen to determine the position and size of underlying structures.
- Do not palpate the abdomen when pulsations are present, in a client who had an organ transplant, or when a Wilm’s tumor is suspected.
- Palpate several areas in each quadrant of the abdomen using a systematic sequence.
- Use light palpation; press down 1 to 2 cm with a slight circular motion.
- Normal findings: Abdomen is soft, not tender, and without palpable masses.
- Deviations: Tenderness, guarding, and rigidity may indicate peritonitis; presence of masses.
10. Assess the anus and perianal area via inspection for color, intactness, and presence of lesions and via touch for the anal reflex.
- Normal findings.
- Color slightly darker than color of buttocks.
- Intact skin that is coarser and moister than perianal skin; absence of lesions.
- Puckering of anus when touched with gloved finger (anal reflex).
- Deviations.
- Fissures, lesions, warts, hemorrhoids, bleeding, or rectal prolapse.
- Lack of anal tone.
C. Characteristics of stool
1. Characteristics of stool are influenced by factors such as dietary and fluid intake, exercise, medications, and disease processes.
2. Characteristics of stool include color, consistency, quantity, shape, odor, and constituents.
III. Diagnostic Tests and Related Nursing Care
Diagnostic tests may be prescribed by the primary healthcare provider to provide information regarding a client’s gastrointestinal functioning. The tests presented mainly are prescribed to support a medical diagnosis. Nurses must understand these tests because some of them require the nurse to collect a specimen, others require nursing interventions before and after the test, and all of them require client teaching.
A. Stool examination
1. Commonalities of nursing care for obtaining stool specimens.
- Perform hand hygiene, and wear clean gloves.
- Instruct the client to defecate in a clean, dry bedpan or container under the toilet seat.
- Use medical aseptic technique to collect 1 inch of formed stool or 15 to 30 mL of liquid stool.
- Ensure that the specimen is not contaminated with urine, water, or toilet paper.
- Use a preservative if required.
- Place the labeled container with the specimen into a biohazard, fluid-impervious bag; include appropriate label and laboratory forms.
- Note on the label if the client is menstruating.
- Send the specimen to the laboratory promptly because bacteriological changes may alter test results if testing is delayed.
2. Gross and microscopic stool examination in the laboratory.
- Gross examination: Assesses stool for consistency, color, presence of blood, mucus, excess fat, and pus.
- Microscopic examination: Identifies constituents, such as WBCs, unabsorbed fat, and parasites.
3. Culture and sensitivity.
- Culture assesses stool for presence of pathogens.
- Sensitivity identifies the most effective antibiotics.
- Obtain a specimen using sterile technique.
- Place the specimen in a sterile container.
4. Occult blood (guaiac, Hemoccult).
- Assesses stool for microscopic amounts of blood in feces.
- Teach the client to avoid red meat, poultry, fish, vitamin C, aspirin, and nonsteroidal anti inflammatory drugs before the test because these substances can cause false-positive results.
- Ensure that the specimen is not contaminated with menstrual blood.
- Use a commercial kit.
- Apply a thin smear of stool on the designated window of the test packet.
- Apply a reagent on the area following the specific times indicated by the manufacturer.
- Note that a blue color in response to the reagent indicates the presence of occult blood.
- Repeat the test for three consecutive defecations of stool.
5. Ova and parasites.
- Assessment via a stool specimen.
- Assesses stool for the presence of parasites and their eggs.
- Collect several specimens from various sections of the stool.
- Transport the specimen to the laboratory while still warm to maintain viability of the parasites and eggs.
- Tape test for obtaining specimen for presence of pinworm eggs.
- Assesses for pinworm eggs from around the anus.
- Wear clean gloves to protect self from the client’s body fluids and parasites.
- Collect the specimen in the morning as soon as the client awakens.
- Spread the buttocks, press clear cellophane tape against the skin surrounding the anal opening, remove tape immediately, and place it on a slide.
B. Lower GI series (barium enema)
- Fluoroscopic radiologic examination of the colon after a contrast medium is instilled rectally.
- Secure consent for the procedure.
- Teach about and maintain prescribed dietary restrictions, such as providing a clear liquid diet for 24 hours before the test and maintaining nothing-by-mouth (NPO) status for 8 hours before the test.
- Teach about and/or implement bowel prep, such as a laxative, enema, or suppository, the evening before and/or the morning of the test.
- Explain what will be done in the x-ray department: Positioned on left side and barium will be inserted into the rectum; position will be changed from left side, to back, and then prone; fluoroscopy follows progress of the barium and x-rays are taken.
- Encourage increased fluid intake for 24 hours after the procedure to facilitate defecation of barium.
- Administer laxatives or cathartics as prescribed to facilitate expulsion of the barium.
- Monitor stool, which will be chalky white for 24 to 48 hours or until the barium is completely evacuated.
C. Endoscopy
1. Commonalities of nursing care associated with an endoscopy.
- Teach the client about the procedure, and secure consent for the procedure.
- Teach about bowel prep, such as medications, cathartics, and enemas the day before and morning of the procedure to cleanse the bowel.
- Teach about a clear liquid diet for 48 hours before and NPO after midnight the night before the procedure.
- Administer prescribed medications, such as a sedative or anxiolytic, before the procedure.
2. Sigmoidoscopy.
- Insertion of a tubular speculum for examination of the sigmoid colon and rectum.
- Position the client in the knee chest position or on the left side.
- Encourage the client to take deep breaths to reduce discomfort and relax muscles.
- Sit the client up slowly to avoid hypotension after the procedure.
3. Colonoscopy.
- Insertion of a flexible endoscope through the anus to visualize the entire colon.
- Instruct client to arrange transportation home after the procedure and to avoid driving for 24 hours because conscious sedation is used.
- Explain that the scope will be inserted through the anus into the colon and that polyps may be excised, feces suctioned, and a biopsy taken.
- Explain that increased flatus and abdominal cramping may occur after the test because air is inflated into the bowel during the test to promote visualization.
- Monitor vital signs after the procedure because conscious sedation is used during the procedure.
- Instruct client to notify the primary health-care provider if abdominal pain, fever, chills, mucopurulent discharge, or rectal bleeding occur after the test because these signs may indicate bowel perforation, hemorrhage, or infection.
- Instruct client to avoid heavy lifting for a week and high-fiber foods for 48 hours if a polyp was excised or biopsy was taken during the procedure.
IV. Common Human Responses Associated With Bowel Elimination and Related Nursing Care
Diarrhea, constipation, fecal incontinence, hemorrhoids, and flatulence are common human responses related to bowel elimination. It is essential that the nurse understand the clinical manifestations, precipitating factors, and nursing care associated with each human response to better meet clients’ needs associated with each of these responses.
A. Diarrhea
1. Description.
- Diarrhea is when intestinal hypermotility precipitates passage of fluid and unformed stool.
- Frequency of stool occurs three or more times a day.
2. Clinical manifestations.
- Frequent loose stools.
- Abdominal cramps, pain, or urgency.
- Abdominal distention.
- Hyperactive bowel sounds or flatus.
- Anorexia, nausea, and vomiting.
- Blood in the stool (frank, occult).
- Deficient fluid volume: Weight loss; thready pulse; hypotension; decreased tissue turgor; furrows of the tongue; flushed, dry skin and mucous membranes; sunken eyeballs; decreased urine output; atonic muscles; and mental confusion.
- Electrolyte imbalances, such as hyponatremia and hypokalemia.
- Stool possibly positive for causative pathogen or helminthic.
- With Clostridium difficile, characteristic odor and green-colored stool.
3. Precipitating factors.
- Viral, bacterial, or parasitic gastroenteritis.
- Spicy or greasy food.
- Raw seafood.
- Contaminated food and water.
- Excessive dietary fiber.
- Anxiety or other emotional disturbance.
- Drug side effects: Antibiotics suppress normal GI flora; antineoplastics and laxatives irritate the mucous membranes of the intestines, increasing peristalsis.
- Enteral nutrition (nasogastric or gastrostomy); hypertonic formula or too-rapid administration precipitates peristalsis.
- Health problems, such as lactose intolerance, irritable bowel syndrome, malabsorption syndrome, and celiac disease.
- Ingestion of heavy metals, such as lead or mercury.
- Inflammatory bowel diseases, such as ulcerative colitis or Crohn’s disease.
4. Nursing care for clients who have diarrhea.
- Assess the client.
- Stool frequency, amount, and characteristics, such as consistency, color, and odor.
- Signs and symptoms of deficient fluid volume and electrolyte imbalances.
- Recent foreign travel and dietary intake.
- Obtain a stool specimen (e.g., culture and sensitivity, ova and parasite).
- Maintain standard precautions, such as frequent hand hygiene and gloves for perineal care, when assisting with fecal elimination. Institute contact precautions if diarrhea is caused by infection or infestation; wear a gown and gloves.
- Assist with elimination, such as providing privacy and transferring the client to the toilet, commode, or bedpan; use air fresheners discretely.
- Provide perineal care, such as assessing skin for breakdown and using a protective skin barrier.
- Maintain the prescribed diet, such as NPO, clear liquid, full liquid, bland, low fiber, or dairy- or gluten-free.
- Increase oral fluid intake gradually because a large amount can precipitate peristalsis.
- Administer prescribed medications, such as antibiotics, antidiarrheals, anti helminthics, enteric bacterial replacements, and electrolytes.
- Administer prescribed IV fluids.
- Provide health teaching.
- Discourage intake of spicy and fatty foods; caffeine; and high-fiber foods, such as whole grains, raw fruits and vegetables, figs, and prunes.
- Discourage intake of hot and cold fluids because they stimulate peristalsis.
- Encourage foods high in sodium, such as tomatoes and bouillon, and potassium, such as bananas, oranges, apricots, and potatoes.
- Teach correct handling and refrigeration of food.
- Clean surfaces with hot water and soap after preparing raw chicken.
- Provide adequate refrigeration of perishable foods, such as milk and dairy products and foods containing mayonnaise; discard expired eggs
- Document assessments, interventions, and client responses.
B. Constipation
1. Description.
- Constipation is intestinal hypomotility that precipitates two or fewer stools a week and hard, dry feces.
- Obstipation is intractable constipation.
- Perceived constipation: Self-diagnosed constipation.
- Fecal impaction is hard, dry stool firmly wedged in the rectal vault that cannot be passed.
2. Clinical manifestations.
- Hypoactive bowel sounds.
- Distended abdomen.
- Rectal pressure or back pain.
- Straining at stool.
- Anorexia.
- Blood-streaked stool.
- Possible fluid and electrolyte imbalances.
- For fecal impaction: Oozing diarrhea around an impaction; fecal mass confirmed by digital examination.
3. Precipitating factors.
- Elimination habits.
- Laxative or enema misuse.
- Urge ignored because of inaccessible bathroom or anticipation of pain because of hemorrhoids, rectal or anal fissures, or other rectal or anal problems.
- Inadequate fluid intake (less than 2 L/day).
- Inadequate intake of fiber (e.g., whole grains, fruits, vegetables) in diet.
- Side effects of opioids, iron, or anesthesia.
- Developmental level.
- Child: Stool withholding behavior.
- Pregnant woman: Uterine compression of intestine, decreasing peristalsis.
- Older adult: Decreased peristalsis.
- Inadequate physical activity.
- Presence of mechanical obstruction or anal lesion.
- Weak abdominal muscles; pelvic floor dysfunction or damage.
- Anxiety or other emotional disturbance.
- Cultural and family health beliefs, such as daily use of a laxative or cathartic.
4. Nursing care for clients who have constipation.
- Assess stool for frequency, amount, color (e.g., greenish black due to iron intake), and shape (e.g., ribbon shape due to obstruction, pencil shape due to mucosal inflammation).
- Assess for perceived constipation by asking if laxatives or cathartics are used daily.
- Maintain standard precautions, such as performing frequent hand hygiene and wearing gloves when providing perineal care and assisting with fecal elimination.
- Assist with elimination, such as providing privacy and encouraging the client to sit in an upright position, lean forward at the hips, apply manual pressure over the abdomen, and bear down while exhaling to prevent straining.
- Encourage toileting after meals or offer a warm drink before a client’s attempt to defecate to take advantage of the gastrocolic reflex. The gastrocolic reflex is the initiation of peristaltic waves when food enters the stomach, particularly when the stomach is empty.
- Administer prescribed medications, such as laxatives and cathartics.
- Administer prescribed enemas, such as oil retention, small-volume hypertonic solution, tap water, or soapsuds.
- Provide health teaching.
- Encourage intake of high-fiber foods, such as whole grains, fruits, and vegetables.
- Discourage intake of binding foods, such as bananas and rice.
- Encourage increased fluid intake, activity, and exercise.
- Encourage consistent bowel habits, and teach the client to respond to the urge to defecate.
- Teach that a daily bowel movement is not always realistic and laxatives and cathartics are not advised because it causes dependence.
- Provide perioperative nursing care if surgery is necessary to remove a fecal impaction.
- Document assessments, interventions, and client responses.
C. Fecal incontinence
1. Description.
- Fecal incontinence is the involuntary passage of feces and flatus from the anus.
- Extent of incontinence ranges from occasional episodes of seepage of stool to total loss of control of the passage of stool.
2. Clinical manifestations. a. Inability to control exit of feces from the body. b. Embarrassment due to soiling.
3. Precipitating factors.
- Inability to recognize the urge to defecate or the presence of rectal fullness due to altered thought processes.
- Impaired anal sphincter control or its nerve supply (e.g., brain attack and spinal cord damage).
- Decreased muscle tone.
- Diarrhea.
4. Nursing care for clients who have fecal incontinence.
- Maintain a nonjudgmental environment; understand that incontinence may be viewed by the client as regression.
- Provide privacy and positive reinforcement.
- Provide prompt hygiene care.
- Use an incontinence device, such as Depends; avoid using the word “diaper,” which is demeaning.
- Encourage attempts to defecate (e.g., in the morning, evening, and after meals to take advantage of the gastrocolic reflex).
- Implement and teach the client about a bowel retraining program.
- Follow the client’s usual pattern.
- Follow the schedule exactly.
- Increase fiber in the diet gradually.
- Encourage the intake of eight or more glasses of water daily.
- Administer a prescribed suppository or cleansing enema to empty the bowel to help promote eventual regularity.
D. Hemorrhoids
1. Description.
- Hemorrhoids are engorged, painful, bleeding veins in the lining of the rectum and anus.
- Can be internal or external.
2. Clinical manifestations.
- Rectal pressure, burning, and pain.
- Frank red blood from the anus.
3. Precipitating factors.
- Constipation or straining on defecation.
- Situations that increase venous pressure, such as pregnancy, weightlifting, standing for long periods of time, heart failure, and chronic liver disease.
4. Nursing care for clients who have hemorrhoids.
- Assess the anal area for the extent of swelling.
- Assess levels of rectal pain.
- Provide meticulous perianal hygiene, especially after defecation.
- Administer prescribed medications, such as stool softeners, local anesthetics, and anal lubricants.
- Administer prescribed thermal therapy to the perianal area, such as cold (e.g., cold packs) or heat (e.g., warm compresses and sitz baths).
- Provide health teaching.
- Encourage the intake of high-fiber foods after acute episodes have subsided.
- Encourage the intake of at least 2 L of fluid daily.
- Teach the client to avoid standing or sitting for long periods.
- Provide care related to band ligation, hemorrhoidectomy, sclerotherapy, cryosurgery, infrared photocoagulation, or laser surgery.
E. Flatulence
1. Description.
- Flatus is gas in the stomach and intestines as a natural by-product of digestion that is expelled through the anus.
- Flatulence is excessive gas in the stomach and intestines that leads to distention of these organs precipitating physical discomfort.
2. Clinical manifestations of flatulence.
- Hyperactive bowel sounds.
- Cramping and/or abdominal pain.
- Abdominal distention.
3. Precipitating factors.
- Absent or decreased GI motility due to such factors as inadequate fiber in the diet, immobility, anesthesia, and opioids.
- Gas-forming foods and fluids, such as beans, peas, cabbage, onions, cauliflower, highly spicy foods, milk and milk products, and carbonated beverages.
- Swallowing of air that accompanies the intake of food and fluid.
4. Nursing care for clients who have flatulence.
- Inspect the abdomen for abdominal distention.
- Auscultate bowel sounds for hypoactivity or hyperactivity; be aware that the absence of bowel sounds may indicate cessation of peristalsis (such as from adynamic ileus, postoperative ileus, or paralytic ileus).
- Encourage activity.
- Encourage in-bed activity when on bedrest, such as turning from side to side.
- Increase ambulation; progressive ambulation after surgery.
- Administer prescribed medications, such as anti flatulences or bulk cathartics.
- Insert a lubricated rectal tube as prescribed (4 to 5 inches for 15 to 20 minutes every 3 to 4 hours) to promote the expulsion of gas.
- Administer a return-flow enema (Harris flush, Harris drip).
- Teach to avoid gas-forming foods and fluids.
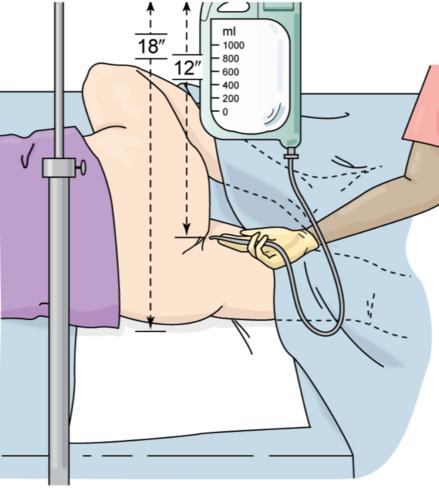
V. Enemas
An enema is the instillation of solution into the intestine via the anus and rectum. The administration of an enema is a dependent function of the nurse that requires a prescription from a primary health-care provider. There are various types of enemas, each with its own distinct purpose because of the way in which it precipitates a response in the body. Commonalities of nursing care for clients receiving an enema are presented here as well as nursing care specific to each type of enema.
A. Commonalities of nursing care for clients receiving an enema
1. Maintain standard precautions, such as performing hand hygiene and wearing gloves.
2. Explain the procedure to the client.
3. Prepare the equipment.
- Fill the enema container with solution that is 105°F or obtain a prefilled hypertonic enema product.
- Flush the tubing or nozzle to remove air. c. Lubricate the tip of the tube or nozzle with water-soluble jelly.
4. Provide privacy, such as by closing the door, pulling the curtain, draping the client, and ensuring that the bathroom is accessible and reserved.
5. Place the client in left-lateral or left Sims’ position to allow the solution to flow by gravity along the natural curve of the sigmoid.
- For small-volume enemas (e.g., hypertonic, oil retention): Insert the probe attached to the container its full length into the anus slowly.
- Large-volume enemas (e.g., tap water, soapsuds): Insert the rectal tube into the anus slowly, 3 to 4 inches for an adult.

6. Interrupt the flow of solution if abdominal pain or cramping occurs; resume the flow when the client states the feeling has subsided.
7. Encourage the client to retain the fluid as long as possible to promote maximum evacuation.
8. Assist the client to a commode or toilet or assist the client onto a bedpan (regular or fracture bedpan) when a client is on bedrest or is unable to exit the bed.
- Begin with the client in the supine position.
- Turn the client on the side or have the client flex the hips and knees and lift the pelvis up off the bed.
- Position the closed end of a regular bedpan or the closed, flat end of a fracture bedpan against the buttock.

- Assist the client to return to the supine position while the nurse holds the bedpan in place.
- Raise the side rails.
- Raise the head of the bed to a comfortable height for the client.
- Position a call bell within easy reach.
- Remain close to the client during evacuation because it may cause dizziness, which is a safety concern.
- Provide perineal hygiene care after the procedure.
- Monitor for therapeutic effect (fecal returns) and untoward results (abdominal distension, rectal bleeding); notify the primary health-care provider if untoward effects occur.
- Document client responses.
VI. Bowel Diversions
Because of a disease process or injury to the bowel, a client may require partial or total, temporary or permanent, surgical removal of the bowel and the creation of a bowel diversion to permit evacuation of intestinal wastes. There are many commonalities of nursing care for clients with bowel diversions, but specific nursing care relates to the differences in the consistency of the fecal discharge (effluent), the type of appliance required, and factors that determine the need for intestinal irrigation.
A. Types of bowel diversion
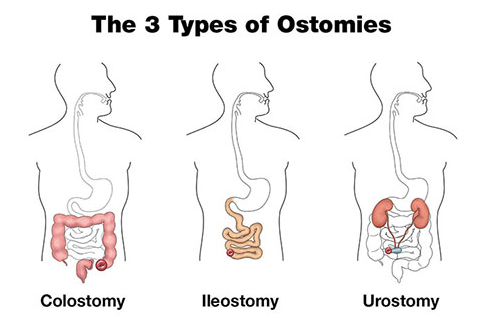
Colostomy.
- A colostomy is the formation of an opening (stoma) between the colon and the surface of the abdomen to permit feces to exit the body from the large intestine.
- Stoma in ascending colon: Liquid stool collected in an appliance.
- Stoma in transverse colon: Semisolid stool collected in an appliance.
- Stoma in descending or sigmoid colon: Solid stool collected in an appliance; may be controlled by daily intestinal irrigations with effluent eliminated in the toilet.
2. Ileostomy.
- An ileostomyis the formation of an opening (stoma) between the ileum and the surface of the abdomen to permit feces to exit the body from the small intestine.
- Typical ileostomy: Liquid stool collected in an appliance.
- Continent Kock pouch: Tube inserted into an external stoma empties an internal reservoir of liquid stool; external pouch unnecessary.
- Ileal-anal anastomosis: Procedure that preserves evacuation through the anus, but evacuation is spontaneous rather than voluntary; liquid stool.
B. Nursing care for clients with a bowel diversion
1. Assess the stoma, which should be deep pink or brick red, shiny, and moist; a pale, purple, or black stoma indicates ischemia and the primary health-care provider should be notified immediately.

2. Assess for bowel sounds and the presence of distention; motility generally returns 3 to 6 days after surgery.
3. Assess the amount, consistency, and characteristics of stool.
4. Change the appliance every 3 to 5 days or as needed; note that many ostomy supplies are available on the market
- Clean the area with soap and water.
- Use a protective barrier on the skin under the appliance.
- Apply an antifungal agent on the skin under the appliance if prescribed.
- Measure and then apply the appliance with a 1/8-inch clearance to avoid stoma damage or skin exposure to stool.

5. Empty the bag when it is half full to avoid excessive tension on the appliance interfering with the integrity of the adhesive resulting in leakage of stool.
6. Refer the client to the United Ostomy Association or an enterostomal therapist.
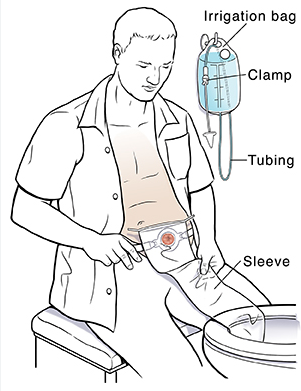
7. Irrigate a distal colostomy
- Irrigate at the same time every day; note that the procedure may take as long as 60 minutes.
- Ensure privacy and adequate access to the bathroom.
- Prepare the irrigating bag with 300 to 1,000 mL of irrigating solution, as prescribed.
- Ensure the irrigating solution is at or slightly above body temperature.
- Flush the solution through the tubing to expel air (priming).
- Lubricate the cone at the end of the tubing.
- Position the client on a toilet or in a side-lying position in bed.
- Place the irrigating sleeve over the stoma.
- Insert the lubricated cone through the opening of the sleeve and gently into the stoma in the direction of the lumen; hold the cone in place during the inflow of solution.
- Stop the procedure and notify the primary healthcare provider if resistance occurs when inserting the cone.
- Shut off the flow of solution if the client experiences cramping; restart the flow once cramping subsides.
- Remove the cone and tubing when the inflow of solution is complete; allow at least 30 minutes for evacuation through the sleeve into the toilet or bedpan.
- Provide hygiene.
- Apply an appliance.
- Document the results and the client’s response.
VII. Medications That Affect Bowel Elimination
When a person is diagnosed with a GI problem, the primary health-care provider can prescribe appropriate medications, depending on the client’s need. The most common medications affecting fecal elimination include antidiarrheals, cathartics and laxatives, and anti flatulents. Additional medications, such as antacids, antiemetics, and antisecretory agents, usually are prescribed for problems interfering with nutrition, but they indirectly influence the GI tract. Nurses should know the mechanisms of action, therapeutic and nontherapeutic effects, and nursing care related to the common medications that are specifically designed to address a client’s GI needs.
A. Antidiarrheals
B. Laxatives
C. Antiflatulent






