Integumentary System
Diagnostic Tests
Skin biopsy is the collection of a small piece of skin tissue for histopathological study; methods include punch, excisional, and shave.
Pre-Op Care:
- Verify informed consent has been obtained.
- Cleanse site as prescribed.
Post-Op Care:
- Place specimen in the appropriate container; send to laboratory for analysis.
- Use aseptic technique
- Assess the biopsy site for bleeding and signs infection.
- Keep dressing clean and dry.
Skin/wound cultures a small skin culture sample is obtained with a sterile applicator and the appropriate type of culture tube (e.g.,bacterial or viral). Methods include scraping, punch biopsy, and collecting fluid.
Post-Op Care:
- Viral culture is placed immediately on ice.
- Send sample immediately to the laboratory.
Candida Albicans a superficial fungal infection of the skin and mucous membranes.
Areas of occurrence: skin folds, perineum, vagina, axilla, and under the breasts.
Nursing Interventions:
- Teach the client to keep skin fold areas clean and dry.
- Provide frequent mouth care; avoid irritating products (alcohol containing mouthwash, liquors)
- Provide food and fluids that are tepid in temperature and nonirritating to mucous membranes.
- Antifungal medications.
Herpes Zoster (Shingles) occur in a segmental distribution on the skin area along the infected nerve and show up after several days of discomfort in the area.
Signs and Symptoms:
- Unilaterally clustered skin vesicles on the trunk, thorax, or face
- Fever, malaise
- Burning and pain
- Paresthesia
- Pruritus
Nursing Interventions:
- Isolation; use standard precaution, contact precaution
- Assess neurovascular status and seventh cranial nerve function; Bell’s palsy is a complication.
- Prevent scratching and rubbing the affected area.
- The zoster vaccine (live), the vaccination for shingles, is recommended for adults 60 years of age and older.
Methicillin-Resistant Staphylococcus aureus (MRSA) is contagious and is spread to others by direct contact with infected skin or infected articles; for the client with MRSA, the infection can also be spread to other parts of the body.
Nursing Interventions:
- Maintain standard precautions and contact precautions.
- Monitor the client closely for signs of further infection.
- Administer antibiotic therapy.
- Hand washing and practicing good personal hygiene.
- Avoiding sharing of personal items.
- Obtain blood cultures, sputum cultures, and urine cultures.
Erysipelas and Cellulitis
Erysipelas is an acute, superficial, rapidly spreading inflammation of the dermis and lymphatics caused by group A Streptococcus; enters the tissue via an abrasion, bite, trauma, or wound. Cellulitis is an infection of the dermis and underlying hypodermis.
Signs and Symptoms:
- Pain and tenderness
- Erythema and warmth
- Edema
- Fever
- Promote rest of the affected area.
- Apply warm compresses
- Apply antibacterial dressings, ointments, or gel
*Culture before antibiotics
Poison Ivy, Poison Oak and Poison Sumac a dermatitis that develops from contact with urushiol from poison ivy, oak, or sumac plants.

Signs and Symptoms:
- Papulovesicular lesions
- Severe pruritus
Nursing Interventions:
- Cleanse the skin
- Administer antihistamines
- Apply cool, wet compresses to relieve the itching.
- Apply topical or glucocorticoid products
- prescribed.
Psoriasis is a chronic, noninfectious skin inflammation occurring with remissions and exacerbations, involving keratin synthesis that results in psoriatic patches.
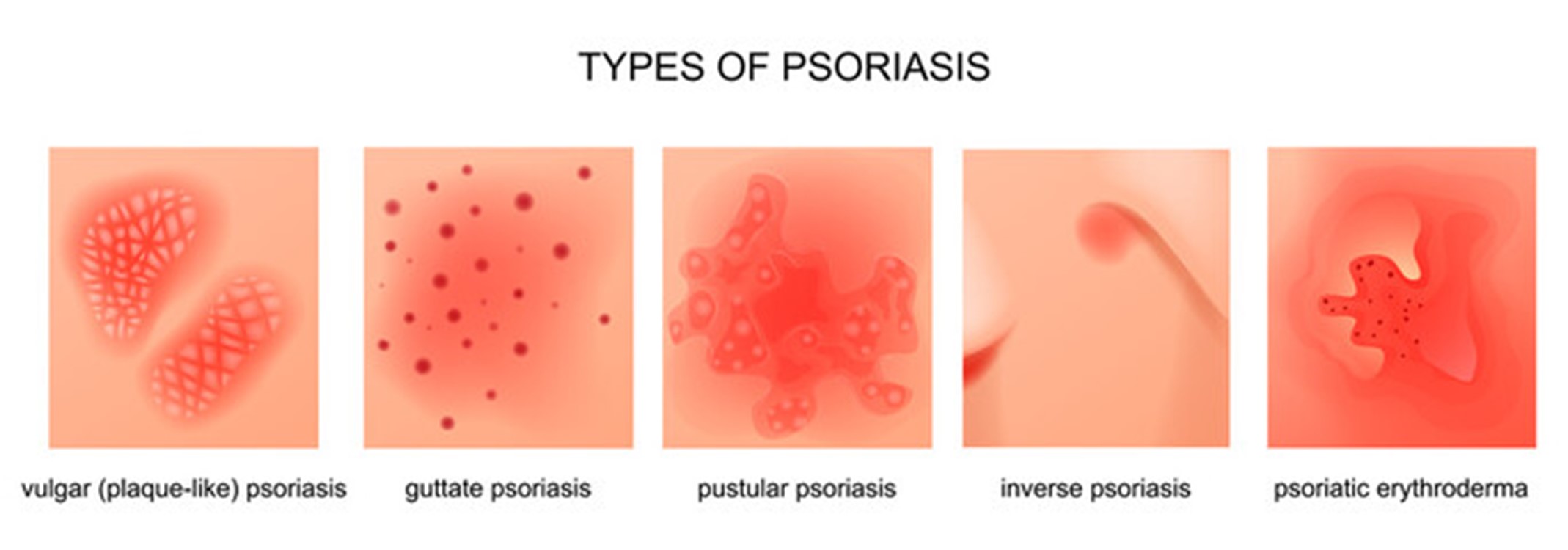
*Koebner phenomenon is the development of psoriatic lesions at a site of injury, such as a scratched or sunburned area.
Signs and Symptoms:
- Pruritus
- Shedding: Silvery-white scales on a raised, reddened, round plaque
- Yellow discoloration, pitting, and thickening of the nails
- Joint inflammation with psoriatic arthritis
Nursing Interventions:
- Instruct the client not to scratch the affected areas and to keep the skin lubricated .
- Monitor signs and symptoms of infection.
- Instruct the client to wear light cotton clothing over affected areas.
Pressure Ulcer occurs when tissue is compressed which restricts blood flow to the skin, which can result in tissue ischemia, inflammation, and necrosis.
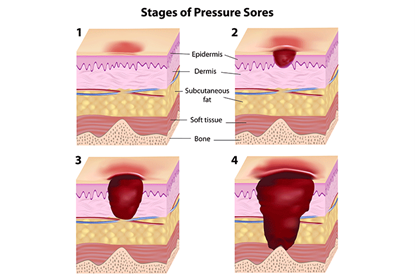
CAUTION! Avoid direct massage to a reddened skin area because massage can damage the capillary beds and cause tissue necrosis.
Nursing Interventions:
- Institute measures to prevent pressure ulcers, such as appropriate positioning, using pressure relief devices, ensuring adequate nutrition, and developing a plan for skin cleansing and care.
- Keep the client’s skin dry and the sheets wrinkle free.
- Use creams and lotions to lubricate the skin and a barrier protection ointment for the incontinent client.
- Turn and reposition the immobile client every 2 hours.
- Provide active and passive range of motion exercises at least every 8 hours.
Other treatment options:
- Electrical stimulation (increases blood vessel growth and stimulates granulation)
- Vacuum assisted wound closure (removes infectious material from the wound and promotes granulation)
- Hyperbaric oxygen therapy (administration of oxygen under high pressure)
Burn Injuries
PRIORITY NURSING ACTIONS! "ABC"
- Assess for airway patency.
- Administer oxygen as prescribed.
- Obtain vital signs.
- Initiate an intravenous (IV) line and begin fluid replacement as prescribed.
- Elevate the extremities if no fractures are obvious.
- Keep the client warm and place the client on NPO (nothing by mouth) status.
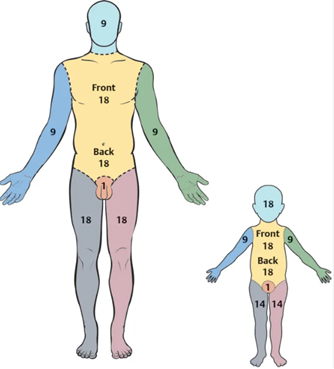
RULE OF NINE
Classification of burns:
Nursing interventions:
Correct fluid and electrolyte imbalance:
-(First 24-48 hr) emergent/resuscitation phase
-Administer LR and plasma (rapid in fusion for the first 8 hours)
- (2-5 days) intermediate phase
- Packed RBCs, strict intake and output
- IV hydration, monitor vitals, labs, weight
Promote healing:
- Wound care and debridement
- Topical antibacterial medications
- Grafting and escharotomy
Nutritional support:
- High calorie, protein and carb
- NG tube
- TPN therapy if ordered
- Vitamin supplementation
Pain management:
- Morphine IV
Prevent immobility:
- PT/OT
- ROM exercises
- Turn Q2hr






