Musculoskeletal Disorders
Diagnostic Tests
Radiography and magnetic resonance imaging (MRI) are commonly used procedures to diagnose disorders of the musculoskeletal system.
Nursing Interventions:
- Handle injured areas carefully and support extremities above and below the joint.
- Remove any radiopaque and metallic objects, such as jewelry.
- Shield the client’s testes, ovaries, or pregnant abdomen.
- NO to pregnant or expecting mothers.
- Inform that the radiation from radiography is minimal and not dangerous.
- *Administer analgesics as prescribed before the procedure.
Arthrocentesis is used to diagnose joint inflammation and infection; involves aspirating synovial fluid, blood, or pus via a needle inserted into a joint cavity.
Nursing Interventions:
- Obtain informed consent
- Apply an elastic compression bandage post procedure
- Use ice to decrease pain and swelling.
- Administer analgesics as prescribed.
- Pain can continue for up to 2 days after administration of corticosteroids into a joint.
- Instruct the client to rest the joint for 8 to 24 hours post procedure.
Arthroscopy provides an endoscopic examination of various joints; articular cartilage abnormalities can be assessed, loose bodies removed, and the cartilage trimmed.
Nursing Interventions:
- Fasting: 8 to 12 hours before the procedure.
- Obtain informed consent.
- Assess the neurovascular status of the affected extremity.
- An elastic compression bandage should be worn post procedure for 2 to 4 days.
- Instruct the client that walking with weight bearing usually is permitted after sensation returns but to limit activity for 1 to 4 days.
- Instruct the client to elevate the extremity as often as possible for 24 hours post-op.
- Place ice on the site.
Bone scan is used to identify, evaluate, and stage bone cancer before and after treatment; it is also used to detect fractures.
Nursing Interventions:
- NPO prior to the procedure.
- Obtain informed consent.
- Remove all jewelry and metal objects.
- Increase OFI after the procedure to eliminate excess isotopes
- 1 to 3 hours after the injection, have the client void before the scanning procedure is completed.
Bone or muscle biopsy may be done during surgery or through aspiration or punch or needle biopsy.
Nursing Interventions:
- Obtain informed consent
- Monitor for bleeding, swelling, hematoma, or severe pain.
- Elevate the site for 24 hours following the procedure.
- Apply ice packs.
- Monitor for signs of infection.
Electromyography (EMG) measures electrical potential associated with skeletal muscle contractions.
Nursing Interventions:
- Obtain informed consent.
- Instruct the client that the needle insertion is uncomfortable.
- Do not take any stimulants or sedatives for 24 hours before the procedure.
- Inform the client that slight bruising may occur at the needle insertion sites.
Injuries
Strains are an excessive stretching of a muscle or tendon.
Nursing Interventions:
- Apply warm and cold compress
- Limit activity
- Medicate for pain and muscle relaxants
Sprains are characterized by pain and swelling.
Nursing Interventions:
" R-I-C-E "
- Rest the affected site
- Apply Ice compress
- Apply Compression bandage
- Elevate legs
- *Casting may require
Rotator cuff injuries is characterized by shoulder pain and the inability to maintain abduction of the arm at the shoulder (drop arm test).
Nursing Interventions:
- Apply ice to heat compress.
- Apply arm sling.
- Administer NSAIDs as prescribed.
Fractures a break in the continuity of the bone caused by trauma, twisting because of muscle spasm or indirect loss of leverage, or bone decalcification and disease.
Signs and Symptoms:
" BROKEN "
- Bruising with pain and swelling
- Reduced movement
- Odd appearance
- Kracking sounds
- Edema and erythema on sites
- Neurovascular impairment (decrease in sensation, temperature changes, loss of function etc.)
Types of Fractures:
Closed or Simple: Skin over the fractured area remains intact.
Comminuted: The bone is splintered or crushed, creating numerous fragments.
Complete: The bone is separated completely by a break into 2 parts.
Compression: A fractured bone is compressed by other bone.
Depressed: Bone fragments are driven inward.
Greenstick: One side of the bone is broken and the other is bent; these fractures occur most commonly in children.
Impacted: A part of the fractured bone is driven into another bone.
Incomplete: Fracture line does not extend through the full transverse width of the bone.
Oblique: The fracture line runs at an angle across the axis of the bone.
Open or Compound: The bone is exposed to air through a break in the skin, and soft tissue injury and infection are common.
Pathological: The fracture results from weakening of the bone structure by pathological processes such as neoplasia; also called spontaneous fracture.
Spiral: The break partially encircles bone. Transverse: The bone is fractured straight across.
Nursing Interventions:
- Immobilize the affected extremity with a cast or splint.
- Assess the neurovascular status of the extremity.
- Interventions for a fracture: Reduction, fixation, traction, cast
Traction is the exertion of a pulling force applied in 2 directions to reduce and immobilize a fracture; provides proper bone alignment and reduces muscle spasms.
Nursing Interventions:
" TRACTION "
- Temperature (infection, extremity)
- Ropes hang freely
- Alignments
- Circulation check
- Type and location of fracture
- Increase OFI
- Overhead trapeze
- No weight on bed or floor
Types of tractions:
Skeletal traction is applied mechanically to the bone with pins, wires, or tongs; typical weight for skeletal traction is 25 to 40 lb (11 to 18 kg).
Nursing Interventions:
- Monitor color, motion, and sensation of the affected extremity.
- Monitor the insertion sites for redness, swelling, drainage, or increased pain.
- Provide insertion site care as prescribed.
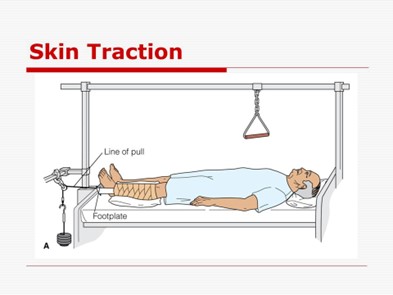
Skin traction is applied by using elastic bandages or adhesive, foam boot, or sling.
Cervical Skin Traction relieves muscle spasms and compression in the upper extremities and neck.

Nursing Interventions:
- Uses ahead halter and chin pad to attach the traction.
- Use powder to protect the ears from friction rub.
- Elevate the head of the bed 30 to 40 degrees.
- Attach the weights to a pulley system over the head of the bed.
Buck’s(extension) skin traction is used to alleviate muscle spasms and immobilize a lower limb by maintaining a straight pull on the limb with the use of weights.
Nursing Interventions:
- Apply boot appliance to the attach to the traction.
- Not more than 8 to 10 lb (3.5 to 4.5 kg) of weight should be applied as prescribed.
- Elevate the foot of the bed to provide the traction.
Pelvic Skin Traction is used to relieve low back, hip, or leg pain or to reduce muscle spasm.
Nursing Interventions:
- Apply the traction belt snugly over the pelvis and iliac crest and attach to the weights.
- Use measures as prescribed to prevent the client from slipping down in bed.
Balanced Suspension Traction Used to approximate fractures of the femur, tibia, or fibula; produced by a counterforce other than the client.
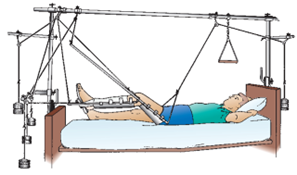
Nursing Interventions:
- Position the client in a low Fowler’s position on either the side or the back.
- Maintain a 20-degree angle from the thigh to the bed.
- Protect the skin from breakdown.
- Provide pin care (if pins are used with the skeletal traction)
- Clean the pin sites with sterile normal saline and hydrogen peroxide or povidone-iodine.
Casts are used to immobilize bones and joints into correct alignment after a fracture or injury using plaster, fiberglass, or air casts.
Nursing Interventions:
- Keep the cast and extremity elevated.
- Allow a wet plaster cast 24 to 72 hours to dry (synthetic casts dry in 20 minutes).
- Handle a wet plaster cast with the palms of the hands (not fingertips) until dry.
- Turn the extremity every 1 to 2 hours, unless contraindicated.
- A hair dryer can be used on a cool setting to dry
- Monitor closely for circulatory impairment (compartment syndrome)
- Maintain smooth edges around the cast to prevent crumbling of the cast material.
- Monitor for signs of infection such as increased temperature, hot spots on the cast, foul odor, or changes in pain.
- Instruct the client not to stick objects inside the cast.
- Teach the client to keep the cast clean and dry.
- Instruct the client in isometric exercises to prevent muscle atrophy.
Caution! Monitor a casted extremity for circulatory impairment such as pain, swelling, discoloration, tingling, numbness, coolness, or diminished pulse. Notify the HCP immediately if circulatory compromise occurs.
Complications of Fractures:
Fat Embolism
- Notify the health care provider (HCP).
- Administer oxygen.
- 3. Administer intravenous (IV) fluids
- Monitor vital signs and respiratory status.
- Prepare for intubation and mechanical ventilation if necessary
- Follow up on results of diagnostic tests such as chest x-ray or CT scan
- Documentation
Pulmonary Embolism is caused by the movement of foreign particles (blood clot, fat, or air) into the pulmonary circulation.
Signs and Symptoms:
- Restlessness and apprehension
- Sudden onset of dyspnea and chest pain
- Cough, hemoptysis, hypoxemia, or crackles
Nursing Interventions:
- Notify the HCP immediately
- Administer oxygen, intravenous (IV), anticoagulant therapy.
Compartment Syndrome occurs when pressure increases within 1 or more compartments, leading to decreased blood flow, tissue ischemia, and neurovascular impairment.
Note: * Neurovascular damage may be irreversible if not treated within 4 to 6 hours.
Signs and Symptoms:
" 5Ps "
- Pain (increasing) in the limb.
- Pale, dusky, or edematous distal tissues.
- Pain with passive movement
- Paresthesia
- Pulselessness (late sign)
Nursing Interventions:
- Notify the HCP immediately
- Elevate the affected extremity.
- Fasciotomy to relieve pressure and restore tissue perfusion.
- Loosen tight dressings or bivalve restrictive cast as prescribed.
Osteomyelitis (inflammatory response in bone tissue) can be caused by the introduction of organisms into bones leading to localized bone infection.
Signs and Symptoms:
- Tachycardia and fever
- Erythema and pain in the area
- Leukocytosis and elevated ESR level
Nursing Interventions:
- Notify the HCP
- Prepare to initiate aggressive, long-term IV antibiotic therapy.
Avascular necrosis occurs when a fracture interrupts the blood supply to a section of bone, leading to bone death.
Signs and Symptoms:
- Pain
- Decreased sensation
Nursing Interventions:
- Notify the HCP if pain or numbness occurs.
- Prepare the client for removal of necrotic tissue.
Crutch Walking
*This video includes all the things you need to learn regarding the use of crutches.
Please click the " Link " below to watch this video.
Nursing Interventions:
- The distance between the axillae and the arm: 2 to 3 finger widths in the axilla space.
- The elbows should be slightly flexed, 20 to 30 degrees, when the client is walking.
- When ambulating with the client, stand on the affected side.
- Look up and outward when ambulating and to place the crutches 6 to 10 inches (25.5 cm) diagonally in front of the foot.
- Instruct the client to stop ambulation if numbness or tingling in the hands or arms occurs.
Hemicanes or quadripod canes are used for clients who have the use of only 1 upper extremity.

Nursing Interventions:
- Position the cane at the client’s unaffected side, with the straight, nonangled side adjacent to the body.
- Position the cane 6 inches (15 cm) from the unaffected client’s side.
Walker
Nursing Interventions:
- Stand adjacent to the client on the affected side.
- Instruct the client to put all 4 points of the walker flat on the floor before putting weight on the hand pieces.
- Instruct the client to move the walker forward, followed by the affected or weaker foot and then the unaffected foot.
Fractured Hip
Types:
1. Intracapsular (femoral head is broken within the joint capsule); Femoral head and neck receive decreased blood supply and heal slowly.
Nursing Interventions:
- Skin traction is applied preoperatively to reduce the fracture and decrease muscle spasms
- Treatment: Total hip replacement or open reduction internal fixation (ORIF) with femoral head replacement.
- To prevent hip displacement postoperatively; avoid extreme hip flexion.
- Extracapsular (fracture is outside the joint capsule) fracture can occur at the greater trochanter or can be an intertrochanteric fracture.
Nursing Interventions:
- Preoperative treatment: Balanced suspension or skin traction
- Surgical treatment: ORIF with nail plate, screws, pins, or wires.
- Postoperative treatment: Monitor for signs of delirium and institute safety measures. Prevent internal or external rotation; avoid extreme hip flexion.
- Elevate the head of the bed 30 to 45 degrees for meals only.
- Avoid weight-bearing on the affected leg.
- Keep the operative leg extended, supported, and elevated (preventing hip flexion)
- Monitor for wound infection or hemorrhage.
- Use antiembolism stockings or sequential compression stockings.
- Avoid crossing the legs and activities that require bending over.
Total knee replacement is the implantation of a device to substitute for the femoral condyles and tibial joint surfaces.
Post-Op Care:
- Monitor surgical incision for drainage and infection.
- Prepare the client for out-of-bed activities as prescribed; avoid leg dangling.
- Weight-bearing with an assistive device is prescribed as tolerated.
- Administer antibiotics if prescribed.
Joint Dislocation injury of the ligaments surrounding a joint, which leads to displacement or separating of the articular surfaces of the joint.
Subluxation incomplete displacement of joint surfaces when forces disrupt the soft tissue that surrounds the joints.
Signs and Symptoms:
- Asymmetry of the contour of affected body parts.
- Pain, tenderness, dysfunction, and swelling
- X-rays are taken to determine joint shifting.
Nursing Interventions:
- Focus of treatment: pain relief, joint support, and joint protection.
- Open or closed reduction is done with a postprocedural joint immobilization.
- Initial activity restriction is followed by gentle range-of-motion activities and a gradual return of activities to normal levels.
Cervical Disk Herniation occurs at the C5 to C6 and C6 to C7 interspaces; causes pain radiation to shoulders, arms, hands, scapulae, and pectoral muscles.
Signs and Symptoms:
- Paresthesia
- Numbness
- Weakness of the upper extremities
Nursing Interventions:
- Bed rest
- Immobilize the cervical area with a cervical collar or brace.
- Apply heat to reduce muscle spasms and apply ice to reduce inflammation and swelling.
- Maintain head and spine alignment.
- Administer analgesics, corticosteroids, sedatives, and anti-inflammatory medications as prescribed.
- Avoid flexing, extending, and rotating the neck.
- Avoid the prone position; maintain in neutral position
Lumbar Disk Herniation most often occurs at the L4 to L5 or L5 to S1 interspace. Pain is relieved by bed rest and aggravated by movement, lifting, straining, and coughing.
Signs and Symptoms:
- Lower back pain radiating to lower limbs down.
- Muscle spasm to lower extremities.
Nursing Interventions:
- Apply heat to decrease muscle spasms and apply ice to decrease inflammation and swelling.
- Instruct the client to sleep on the side, with the knees and hips flexed, and place a pillow between the legs.
- Apply pelvic traction as prescribed to relieve muscle spasms and decrease pain.
- Begin progressive ambulation as inflammation, edema, and pain subside.
- Instruct the client about application techniques for corsets or braces to maintain immobilization and proper spine alignment.
- Instruct about proper body mechanics.
Disk Surgery is used when spinal cord compression is suspected or symptoms do not respond to conservative treatment.
Pre-Op Care:
- Monitor for respiratory difficulty from inflammation or hematoma.
- Encourage coughing, deep breathing, and early ambulation.
- Monitor for hoarseness and inability to cough effectively.
- Assess the surgical dressing; monitor the surgical wound for infection, swelling, redness, drainage, or pain.
- DIET: Soft diet
- Monitor for sudden return of radicular pain; may indicate cervical spine instability.
Post-Op Care:
- Assess the surgical dressing, bleeding, drainage, and surgical drains.
- Monitor lower extremities for sensation, movement, color, temperature, and paresthesia.
- Monitor for urinary retention, paralytic ileus, and constipation.
- DIET: High fiber diet; increase oral fluid intake (OFI)
- Administer opioids and sedatives as prescribed to relieve pain and anxiety.
- Assist regarding the use of back brace or corset and to wear cotton underwear to prevent skin irritation.
- Position: Lie in supine; place a pillow under the neck and slightly flex the knees.
- Avoid spinal flexion or twisting and that the spine should be kept aligned.
- Avoid extreme hip flexion when lying on the side.
- Following disk surgery, instruct the client in correct logrolling techniques for turning and repositioning and for getting out of bed.
Amputation is the surgical removal of a limb or part of the limb.
Post-Op Care:
- Monitor for signs of complications (hemorrhage, infection, phantom limb pain, neuroma, and flexion contractures)
- Mark bleeding and drainage on the dressing if it occurs.
- Evaluate for phantom limb sensation and pain; medicate immediately.
- Do not elevate the residual limb on a pillow.
- First 24 hours: Elevate the foot of the bed to reduce edema; then keep the bed flat to prevent hip flexion contractures,
- After 24 to 48 hours: position the client prone to stretch the muscles and prevent hip flexion contractures.
- Maintain surgical application of dressing, elastic compression wrap, or elastic stump.
- Massage the skin toward the suture line to mobilize scar and prevent its adherence to underlying bone.
- Provide emotional support for the loss of body part.
Interventions for below-knee amputation:
" NAPE "
- Not to hang residual limbs over the edge of the bed.
- Alignment: Discourage long periods of sitting and knee flexion.
- Prone position
- Edema prevention
Interventions for above-knee amputation:
" 2Ps "
- Position in prone
- Prevent internal or external rotation of the limb; use sandbag, rolled towel, or trochanter roll along the outside of the thigh.
Rheumatoid Arthritis (RA) is a chronic systemic inflammatory disease (immune complex disorder); the cause may be related to a combination of environmental and genetic factors; leads to destruction of connective tissue and synovial membrane within the joints.
Signs and Symptoms:
- Inflammation, tenderness, and stiffness of the joints
- Morning stiffness lasting longer than 30 minutes.
- Spongy, soft feeling in the joints
- Low-grade temperature, fatigue, and weakness
- Elevated ESR and positive rheumatoid factor (Reference interval: Negative or < 60 units/mL)
- Synovial tissue biopsy reveals inflammation
Nursing Interventions:
- Provide range-of-motion exercise.
- Splints may be used during acute inflammation to prevent deformity.
- Apply heat or cold therapy as prescribed to joints.
- Avoid weight-bearing on inflamed joints.
- Identify and correct safety hazards in the home.
- Encourage the client to verbalize feelings.
- Assist the client with self-care activities and grooming.
Osteoarthritis (OA) is marked by progressive deterioration of the articular cartilage; causes bone buildup and the loss of articular cartilage in peripheral and axial joints.
Signs and Symptoms:
- Joint pain that diminishes after rest and intensifies after activity.
- Pain occurs with slight motion or even at rest.
- Aggravated by temperature change and climate humidity.
- Difficulty getting up after prolonged sitting.
- Presence of Heberden’s nodes (high) or Bouchard’s nodes (below)
Nursing Interventions:
- Administer medications as prescribed, such as acetaminophen or topical applications, NSAIDs and muscle relaxants.
- Position joints in function position and avoid flexion of knees and hips.
- Prepare the client for corticosteroid injections into joints as prescribed.
- Provide a bed or foot cradle to keep linen off feet and legs until inflammation subsides.
- Avoid large pillows under the head or knees.
- Immobilize the affected joint with a splint or brace until inflammation subsides.
- Apply cold applications as prescribed when the joint is acutely inflamed.
- Instruct the client to balance activity with rest and to participate in an exercise program.
Gout is a systemic disease in which urate crystals deposit in joints and other body tissues, results from abnormal amounts of uric acid in the body.
Types:
- Primary gout results from a disorder of purine metabolism.
- Secondary gout involves excessive uric acid in the blood caused by another disease.
Phases:
- Asymptomatic: Client has no symptoms, but serum uric acid level is elevated.
- Acute: Client has excruciating pain and inflammation of 1 or more small joints, especially the great toe.
- Intermittent: Client has intermittent periods without symptoms between acute attacks.
- Chronic: Results in deposits of urate crystals under the skin, within major organs, such as the kidneys, leading to organ dysfunction.
Signs and Symptoms:
- Swelling and inflammation of the joints, leading to excruciating pain.
- Tophi: Hard, irregularly shaped nodules in the skin containing chalky deposits of sodium urate
- Low-grade fever, malaise, and headache.
- Pruritus from urate crystals in the skin
- Presence of renal stones from elevated uric acid levels
Nursing Interventions:
- DIET: Low-purine diet; avoiding foods such as organ meats, wines, and aged cheese.
- Encourage a high fluid intake of 2000 mL/day.
- Encourage a weight reduction diet.
- Avoid alcohol and starvation diets because they may precipitate a gout attack.
- Increase urinary pH (above 6) by eating alkaline ash foods (i.e., green beans, broccoli).
- Monitor joint range-of-motion ability and appearance of joints.
- Provide heat or cold for local treatments to affected joint as prescribed.
- Administer medications such as analgesic, anti-inflammatory, and uricosuric agents as prescribed.
- Position the joint in mild flexion during acute attack.
Osteoporosis occurs post-menopausal or as a result of a metabolic disorder or calcium deficiency, most commonly in the wrist, hip, and vertebral column.
Types:
Primary osteoporosis
- Most often occurs in postmenopausal women; occurs in men with low testosterone levels
- Risk factors include decreased calcium intake, deficient estrogen, and sedentary lifestyle.
Secondary osteoporosis
- Causes include prolonged therapy with corticosteroids, thyroid-reducing medications, aluminum-containing antacids, or antiseizure medications.
- Associated with immobility, alcoholism, malnutrition, or malabsorption.
Risk Factors for Osteoporosis
▪ Cigarette smoking
▪ Early menopause
▪ Excessive use of alcohol
▪ Family history
▪ Female gender
▪ Increasing age
▪ Insufficient intake of calcium
▪ Sedentary lifestyle
▪ Thin, small frame
▪ White (European descent) or Asian race
Signs and Symptoms:
- Back pain that occurs after lifting, bending, or stooping.
- Pelvic or hip pain, especially with weight-bearing.
- Decline in height from vertebral compression.
- Kyphosis of the dorsal spine, also known as “dowager’s hump”
Nursing Interventions:
- Safety measures
- Clear walkway at home.
- Use side rails to prevent falls.
- Instruct in use of assistive devices such as a cane or walker.
- Use of a firm mattress.
- Move the client gently when turning and repositioning.
- Provide gentle range-of-motion exercises.
- Apply a back brace as prescribed during an acute phase.
- DIET: high in protein, calcium, vitamins C and D, and iron
- Maintain an adequate fluid intake to prevent renal calculi.






