I. NUTRIENTS
A. Carbohydrates
1. Carbohydrates are the preferred source of energy.
2. Sugars, starches, and cellulose provide 4 cal/g.
3. Carbohydrates promote normal fat metabolism, spare protein, and enhance lower gastrointestinal function.
4. Major food sources of carbohydrates include milk, grains, fruits, and vegetables.
5. Inadequate carbohydrate intake affects metabolism.
B. Fats
1. Fats provide a concentrated source and a stored form of energy.
2. Fats protect internal organs and maintain body temperature.
3. Fats enhance absorption of the fat-soluble vitamins.
4. Fats provide 9 cal/g.
5. Inadequate intake of essential fatty acids leads to clinical manifestations of sensitivity to cold, skin lesions, increased risk of infection, and amenorrhea in women.
6. Diets high in fat can lead to obesity and increase the risk of cardiovascular disease and some cancers.
C. Proteins
1. Amino acids, which make up proteins, are critical to all aspects of growth and development of body tissues, and provide 4 cal/g.
2. Proteins build and repair body tissues, regulate fluid balance, maintain acid-base balance, produce antibodies, provide energy, and produce enzymes and hormones.
3. Essential amino acids are required in the diet because the body cannot manufacture them.
4. Complete proteins contain all essential amino acids; incomplete proteins lack some of the essential fatty acids.
5. Inadequate protein can cause protein energy malnutrition and severe wasting of fat and muscle tissue.
NCLEX!!! Major stages of the lifespan with specific nutritional needs are pregnancy, lactation, infancy, childhood, and adolescence. Adults and older adults may experience physiological aging changes, which influence individual nutritional needs.
D. Vitamins
1. Vitamins facilitate metabolism of proteins, fats, and carbohydrates and act as catalysts for metabolic functions.
2. Vitamins promote life and growth processes, and maintain and regulate body functions.
3. Fat-soluble vitamins A, D, E, and K can be stored in the body, so an excess can cause toxicity.
4. The B vitamins and vitamin C are water-soluble vitamins, are not stored in the body, and can be excreted in the urine.

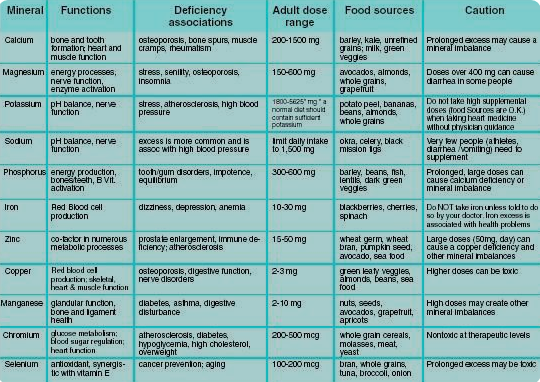
E. Minerals
1. Minerals are components of hormones, cells, tissues, and bones.
2. Minerals act as catalysts for chemical reactions and enhancers of cell function.
3. Almost all foods contain some form of minerals.
4. A deficiency of minerals can develop in chronically ill or hospitalized clients.
5. Electrolytes play a major role in osmolality and body water regulation, acid-base balance, enzyme reactions, and neuromuscular activity.
NCLEX!!! Always assess the client’s ability to eat and swallow and promote independence in eating as much as is possible.
II. MyPlate
A. Provides a description of a balanced diet that includes grains, vegetables, fruits, dairy products, and protein foods (see http://www.choosemyplate.gov/)
B. A nutritionist should be consulted for individualized dietary recommendations.
C. Guidelines
1. Avoid eating oversized portions of foods.
2. Fill half of the plate with fruits and vegetables.
3. Vary the type of vegetables and fruits eaten.
4. Select at least half of the grains as whole grains.
5. Ensure that foods from the dairy group are high in calcium.
6. Drink milk that is fat-free or low fat (1%).
7. Eat protein foods that are lean.
8. Select fresh foods over frozen or canned foods.
9. Drink water rather than liquids that contain sugar.
NCLEX!!! Always consider the client’s cultural and personal choices when planning nutritional intake.
III. THERAPEUTIC DIETS
A. Clear liquid diet
1. Indications
a. Clear liquid diet provides fluids and some electrolytes to prevent dehydration.
b. Clear liquid diet is used as an initial feeding after complete bowel rest.
c. Clear liquid diet is used initially to feed a malnourished person or a person who has not had any oral intake for some time.
d. Clear liquid diet is used for bowel preparation for surgery or diagnostic tests, as well as postoperatively and in clients with fever, vomiting, or diarrhea.
e. Clear liquid diet is used in gastroenteritis.
2. Nursing considerations
a. Clear liquid diet is deficient in energy (calories) and many nutrients.
b. Clear liquid diet is easily digested and absorbed.
c. Minimal residue is left in the gastrointestinal tract.
d. Clients may find a clear liquid diet unappetizing and boring.
e. As a transition diet, clear liquids are intended for short-term use.
f. Clear liquids and foods that are relatively transparent to light and are liquid at body temperature are considered “clear liquids,” such as water, bouillon, clear broth, carbonated beverages, gelatin, hard candy, lemonade, ice pops, and regular or decaffeinated coffee or tea.
g. By limiting caffeine intake, an upset stomach and sleeplessness may be prevented.
h . The client may consume salt and sugar.
i. Dairy products and fruit juices with pulp are not clear liquids.
NCLEX!!! Monitor the client’s hydration status by assessing intake and output, assessing weight, monitoring for edema, and monitoring for signs of dehydration. Each kilogram (2.2 lb) of weight gained or lost is equal to 1 liter of fluid retained or lost.
B. Full liquid diet
1. Indication: May be used as a transition diet after clear liquids following surgery or for clients who have difficulty chewing, swallowing, or tolerating solid foods
2. Nursing considerations
a. A full liquid diet is nutritionally deficient in energy (calories) and many nutrients.
b. The diet includes clear and opaque liquid foods, and those that are liquid at body
temperature.
c. Foods include all clear liquids and items such as plain ice cream, sherbet, breakfast drinks, milk, pudding and custard, soups that are strained, refined cooked cereals, fruit juices, and strained vegetable juices.
d. Use of a complete nutritional liquid supplement is often necessary to meet nutrient needs for clients on a full liquid diet for more than 3 days.
NCLEX!!! Provide nutritional supplements such as those high in protein, as prescribed, for the client on a liquid diet.
C. Mechanical soft diet
1. Indications
a. Provides foods that have been mechanically altered in texture to require minimal chewing
b. Used for clients who have difficulty chewing but can tolerate more variety in texture than a liquid diet offers
c. Used for clients who have dental problems, surgery of the head or neck, or dysphagia (requires swallowing evaluation and may require thickened liquids if the client has swallowing difficulties)
2. Nursing considerations
a. Degree of texture modification depends on individual need, including pureed, mashed, ground, or chopped.
b. Foods to be avoided in mechanically altered diets include nuts; dried fruits; raw fruits and vegetables; fried foods; tough, smoked, or salted meats; and foods with coarse textures.
D. Soft diet
1. Indications
a. Used for clients who have difficulty chewing or swallowing
b. Used for clients who have ulcerations of the mouth or gums, oral surgery, broken jaw, plastic surgery of the head or neck, or dysphagia, or for the client who has had a stroke
2. Nursing considerations
a. Clients with mouth sores should be served foods at cooler temperatures.
b. Clients who have difficulty chewing and swallowing because of dry mouth can increase salivary flow by sucking on sour candy.
c. Encourage the client to eat a variety of foods.
d. Provide plenty of fluids with meals to ease chewing and swallowing of foods.
e. Drinking fluids through a straw may be easier than drinking from a cup or glass; a straw may not be allowed for clients with dysphagia (because of the risk of aspiration).
f. All foods and seasonings are permitted; however, liquid, chopped, or pureed foods or regular foods with a soft consistency are tolerated best.
g. Foods that contain nuts or seeds, which easily can become trapped in the mouth and cause discomfort, should be avoided.
h. Raw fruits and vegetables, fried foods, and whole grains should be avoided.
NCLEX!!! Consider the client’s disease or illness and how it may affect nutritional status.
E. Low-fiber (low-residue) diet
1. Indications
a. Supplies foods that are least likely to form an obstruction when the intestinal tract is narrowed by inflammation or scarring or when gastrointestinal motility is slowed
b. Used for inflammatory bowel disease, partial obstructions of the intestinal tract, gastroenteritis, diarrhea, or other gastrointestinal disorders
2. Nursing considerations
a. Foods that are low in fiber include white bread, refined cooked cereals, cooked potatoes without skins, white rice, and refined pasta.
b. Foods to limit or avoid are raw fruits (except bananas), vegetables, nuts and seeds, plant fiber, and whole grains.
c. Dairy products should be limited to 2 servings a day.
F. High-fiber (high-residue) diet
1. Indication: Used for constipation, irritable bowel syndrome when the primary symptom is alternating constipation and diarrhea, and asymptomatic diverticular disease
2. Nursing considerations
a. High-fiber diet provides 20 to 35 g of dietary fiber daily.
b. Volume and weight are added to the stool, speeding the movement of undigested materials through the intestine.
c. High-fiber foods are fruits and vegetables and whole-grain products.
d. Increase fiber gradually and provide adequate fluids to reduce possible undesirable side effects such as abdominal cramps, bloating, diarrhea, and dehydration.
e. Gas-forming foods should be limited
G. Cardiac diet
1. Indications
a. Indicated for atherosclerosis, diabetes mellitus, hyperlipidemia, hypertension, myocardial infarction, nephrotic syndrome, and renal failure
b. Reduces the risk of heart disease
c. Dietary Approaches to Stop Hypertension (DASH) diet: recommended to prevent and control hypertension, hypercholesterolemia, and obesity
d. The DASH diet includes fruits, vegetables, whole grains, and low-fat dairy foods; meat, fish, poultry, nuts, and beans; and is limited in sugar-sweetened foods and beverages, red meat, and added fats.
2. Nursing considerations
a. Restrict total amounts of fat, including saturated, trans, polyunsaturated, and monounsaturated; cholesterol; and sodium.
b. Teach the client about the DASH diet or other prescribed diet.
H. Fat-restricted diet
1. Indications
a. Used to reduce symptoms of abdominal pain, steatorrhea, flatulence, and diarrhea associated with high intakes of dietary fat, and to decrease nutrient losses caused by ingestion
of dietary fat in individuals with malabsorption disorders
b. Used for clients with malabsorption disorders, pancreatitis, gallbladder disease, and gastroesophageal reflux
2. Nursing considerations
a. Restrict total amount of fat, including saturated, trans, polyunsaturated, and monounsaturated.
b. Clients with malabsorption may also have difficulty tolerating fiber and lactose.
c. Vitamin and mineral deficiencies may occur in clients with diarrhea or steatorrhea.
d. A fecal fat test may be prescribed and indicates fat malabsorption with excretion of more than 6 to 8 g of fat (or more than 10% of fat consumed) per day during the
3 days of specimen collection.
I. High-calorie, high-protein diet
1. Indication: Used for severe stress, burns, wound healing, cancer, human immunodeficiency virus, acquired immunodeficiency syndrome, chronic obstructive pulmonary disease, respiratory failure, or any other type of debilitating
disease.
2. Nursing considerations
a. Encourage nutrient-dense, high-calorie, high protein foods such as whole milk and milk products, peanut butter, nuts and seeds, beef, chicken, fish, pork, and eggs.
b. Encourage snacks between meals, such as milkshakes, instant breakfasts, and nutritional supplements.
NCLEX!!! Calorie counts assist in determining the client’s total nutritional intake and can identify a deficit or excess intake.
J. Carbohydrate-consistent diet
1. Indication: Used for clients with diabetes mellitus, hypoglycemia, hyperglycemia, and obesity
2. Nursing considerations
a. The Exchange System for Meal Planning, developed by the Academy of Nutrition
and Dietetics and the American Diabetes Association, is a food guide that may be
recommended.
b. The Exchange System groups foods according to the amounts of carbohydrates, fats, and proteins they contain; major food groups include the carbohydrate, meat and meat substitute, and fat groups.
c. A carbohydrate consistent diet focuses on maintaining a consistent amount of carbohydrate intake each day and with each meal; also known as “carb counting.” For additional information, refer to: http://www.livestrong.com/article/
436101-the-consistent-carbohydrate-diet-fordiabetics/
d. The MyPlate diet may also be recommended.
K. Sodium-restricted diet
1. Indication: Used for hypertension, heart failure, renal disease, cardiac disease, and liver disease.
2. Nursing considerations
a. Individualized; can include 4 g of sodium daily (no-added-salt diet), 2 to 3 g of
sodium daily (moderate restriction), 1 g of sodium daily (strict restriction), or 500 mg of sodium daily (severe restriction and seldom prescribed)
b. Encourage intake of fresh foods, rather than processed foods, which contain higher amounts of sodium.
c. Canned, frozen, instant, smoked, pickled, and boxed foods usually contain higher
amounts of sodium. Lunch meats, soy sauce, salad dressings, fast foods, soups, and snacks such as potato chips and pretzels also contain large amounts of sodium;
teach patients to read nutritional facts on product packaging regarding sodium content per serving.
d. Certain medications contain significant amounts of sodium.
e. Salt substitutes may be used to improve palatability; most salt substitutes contain large amounts of potassium and should not be used by clients with renal disease.
L. Protein-restricted diet
1. Indication: Used for renal disease and end-stage liver disease
2. The nutritional status of critically ill clients with protein-losing renal diseases, malabsorption syndromes, and continuous renal replacement therapy or dialysis should have their protein needs assessed by estimating the protein equivalent of nitrogen appearance (PNA); a nutritionist should be consulted.
3. Nursing considerations
a. Provide enough protein to maintain nutritional status but not an amount that will
allow the buildup of waste products from protein metabolism (40 to 60 g of protein daily).
b. The less protein allowed, the more important it becomes that all protein in the diet be of high biological value (contain all essential amino acids in recommended proportions).
c. An adequate total energy intake from foods is critical for clients on protein-restricted diets (protein will be used for energy, rather than for protein synthesis).
d. Special low-protein products, such as pastas, bread, cookies, wafers, and gelatin made with wheat starch, can improve energy intake and add variety to the diet.
e. Carbohydrates in powdered or liquid forms can provide additional energy.
f. Vegetables and fruits contain some protein and, for very low-protein diets, these foods must be calculated into the diet.
g. Foods are limited from the milk, meat, bread, and starch groups.
M. Gluten-free diet: A treatment for celiac disease and gluten sensitivity for clients needing the protein fraction “gluten” eliminated from their diet.
NCLEX!!! Fluid restrictions may be prescribed for clients with hyponatremia, severe extracellular cellular volume excess, and renal disorders. Ask specifically about client preferences regarding types of oral fluids and temperature preference of fluids.
N. Renal diet
1. Indication: Used for the client with acute kidney injury or chronic kidney disease and those requiring hemodialysis or peritoneal dialysis.
2. Nursing considerations
a. Controlled amounts of protein, sodium, phosphorus, calcium, potassium, and fluids may be prescribed; may also need modification in fiber, cholesterol, and fat based on individual requirements; clients on peritoneal dialysis usually have diets prescribed that are less restrictive with fluid and protein intake than those on hemodialysis.
b. Most clients receiving dialysis need to restrict fluids.
c. Monitor weight daily as a priority because weight is an important indicator of fluid status.
NCLEX!!! An initial assessment includes identifying allergies and food and medication interactions.
O. Potassium-modified diet
1. Indications
a. Low-potassium diet is indicated for hyperkalemia, which may be caused by impaired renal function, hypoaldosteronism, Addison’s disease, angiotensin-converting enzyme inhibitor medications, immunosuppressive medications, potassium-retaining diuretics, and chronic hyperkalemia.
b. High-potassium diet is indicated for hypokalemia, which may be caused by renal
tubular acidosis, gastrointestinal losses (diarrhea, vomiting), intracellular shifts,
potassium-losing diuretics, antibiotics, mineralocorticoid or glucocorticoid excess
resulting from primary or secondary aldosteronism, Cushing’s syndrome, or exogenous corticosteroid use.
2. Nursing considerations
a. Foods that are low in potassium include applesauce, green beans, cabbage, lettuce, peppers, grapes, blueberries, cooked summer squash, cooked turnip greens, pineapple, and raspberries.
b. Box 11-2 lists foods that are high in potassium.

P. High-calcium diet
1. Indication: Calcium is needed during bone growth and in adulthood to prevent osteoporosis and to facilitate vascular contraction, vasodilation, muscle contraction, and nerve transmission.
2. Nursing considerations
a. Primary dietary sources of calcium are dairy products (see Box 11-2 for food items high in calcium).

b. Lactose-intolerant clients should incorporate nondairy sources of calcium into their diet regularly.
Q. Low-purine diet
1. Indication: Used for gout, kidney stones, and elevated uric acid levels
2. Nursing considerations
a. Purine is a precursor for uric acid, which forms stones and crystals.
b. Foods to restrict include anchovies, herring, mackerel, sardines, scallops, organ meats, gravies, meat extracts, wild game, goose, and sweetbreads.
R. High-iron diet
1. Indication: Used for clients with anemia
2. Nursing considerations
a. The high-iron diet replaces iron deficit from inadequate intake or loss.
b. The diet includes organ meats, meat, egg yolks, whole-wheat products, dark green leafy vegetables, dried fruit, and legumes.
c. Inform the client that concurrent intake of Vitamin C with iron foods enhances absorption of iron.
IV. VEGAN AND VEGETARIAN DIETS
A. Vegan
1. Vegans follow a strict vegetarian diet and consume no animal foods.
2. Eat only foods of plant origin (e.g., whole or enriched grains, legumes, nuts, seeds, fruits, vegetables).
3. The use of soybeans, soy milk, soybean curd (tofu), and processed soy protein products enhance the nutritional value of the diet.
B. Lacto-vegetarian
1. Lacto-vegetarians eat milk, cheese, and dairy foods but avoid meat, fish, poultry, and eggs.
2. A diet of whole or enriched grains, legumes, nuts, seeds, fruits, and vegetables in sufficient quantities to meet energy needs provides a balanced diet.
C. Lacto-ovo-vegetarian
1. Lacto-ovo-vegetarians follow a food pattern that allows for the consumption of dairy products and eggs.
2. Consumption of adequate plant and animal food sources that excludes meat, poultry, pork, and fish poses no nutritional risks.
D. Ovo-vegetarians: The only animal foods that the ovo-vegetarian consumes are eggs, which are an excellent source of complete proteins.
E. Nursing considerations
1. Vegan and vegetarian diets are not usually prescribed but are a diet choice made by a client.
2. Ensure that the client eats a sufficient amount of varied foods to meet nutrient and energy needs.
3. Clients should be educated about consuming complementary proteins over the course of each day to ensure that all essential amino acids are provided.
4. Potential deficiencies in vegetarian diets include energy, protein, vitamin B12, zinc, iron, calcium, omega-3 fatty acids, and vitamin D (if limited exposure to sunlight).
5. To enhance absorption of iron, vegetarians should consume a good source of iron and vitamin C with each meal.
6. Foods eaten may include tofu, tempeh, soy milk and soy products, meat analogs, legumes, nuts and seeds, sprouts, and a variety of fruits and vegetables.
7. Soy protein is considered equivalent in quality to animal protein.
NCLEX!!! Body mass index (BMI) can be calculated by dividing the client’s weight in kilograms by height in meters squared. For example, a client who weighs 75 kg (165 pounds) and is 1.8 m (5 feet, 9 inches) tall has a BMI of 23.15 (75 divided by 1.82¼23.15). From: Potter et al. (2013), p. 1008.
V. ENTERAL NUTRITION
A. Description: Provides liquefied foods into the gastrointestinal tract via a tube
B. Indications
1. When the gastrointestinal tract is functional but oral intake is not meeting estimated nutrient needs
2. Used for clients with swallowing problems, burns, major trauma, liver or other organ failure, or severe malnutrition
C. Nursing considerations
1. Clients with lactose intolerance need to be placed on lactose-free formulas.
XI. PARENTERAL NUTRITION
Parenteral nutrition is the administration of nutrients directly into the bloodstream, bypassing the GI tract. It is used for clients who are incapable of absorbing ample nutrients via the enteral route. Fat or lipid emulsions may be administered as necessary to prevent essential fatty acid deficiency or to add calories to the PN regimen. PN solutions are prepared by a pharmacist using a laminar flow hood to reduce the risk of infection, and medications are never added to the solution. PN solutions and regimens are specifically designed to meet the individual nutritional needs of clients.
A. Types of parenteral nutrition
1. Total parenteral nutrition (TPN).
- For clients with a nonfunctioning GI tract or a high-nutritive demand for a long period of time due to severe trauma, burns, infection, or intense cancer therapy.
- Administered via a central venous catheter (CVC), which surgically perforates the skin; is inserted into a high-flow vein, such as the subclavian or internal jugular; and is advanced into the superior vena cava.
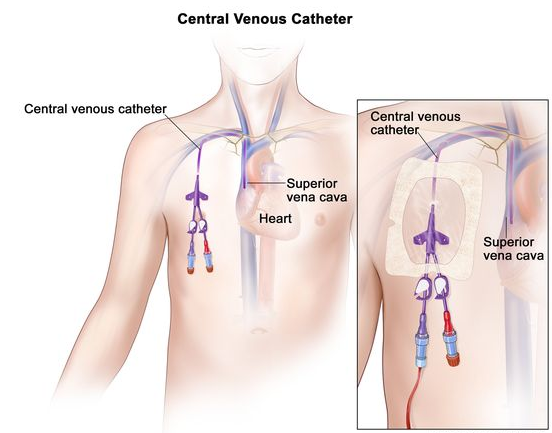
- CVCs have two to four lumens.
- Large central veins are used for TPN because the hypertonic solution is diluted quickly due to the high-flow rate of the circulation; TPN solutions are extremely caustic to peripheral veins.
- Heparin may be added to the parenteral solution to prevent a blood clot from forming on the tip of the catheter.
- Insulin may be added to the parenteral solution because of its high glucose level.
2. Peripheral parenteral nutrition (PPN).
- Administered via a peripherally inserted central catheter (PICC).
- Used for clients who need calories or nutrients beyond what can be taken orally; generally used to supplement oral nutritive intake for a short period of time (generally less than 10 days and for less than 2,000 calories daily).
- PPN solution should not exceed 50% dextrose and 8.5% amino acids at 83 mL/hr.
B. Parenteral nutrition and related nursing care
1. Commonalities of nursing care.
- Ensure PN tube placement is radiographically confirmed before use.
- Verify the prescription (e.g., formula, amount, and rate of infusion), label the PN solution bag (e.g., date, time, and nurse’s initials), and verify the expiration date on the formula.
- Always use an infusion pump to ensure accuracy; dedicate a port for administration of PN solution.
- Refrigerate PN solution until 60 minutes before use.
- Let the solution return to room temperature naturally.
- Cold solutions can cause pain, venous spasm, and hypothermia.
- Do not accelerate warming of a PN solution by placing it in warm water or putting it in a microwave oven because doing so may cause the solution to precipitate, resulting in catheter occlusion or emboli.
- Infuse the PN solution as prescribed; for example, administer slowly initially and increase the rate in increments of 25 mL/hr until the prescribed rate is reached; generally 1 L/day initially and then increased by a prescribed volume daily until the prescribed volume is achieved.
- Monitor for metabolic complications and fluid and electrolyte imbalances because these problems indicate intolerance; the PN may need to be halted, the flow rate decreased, and problems and/or imbalances corrected.
- Monitor blood glucose levels every 6 hours because PN solutions generally are high in glucose; administer insulin coverage as prescribed.
- Monitor the peripheral site for infiltration, thrombophlebitis, and infection. Monitor vital signs for changes indicating a systemic infection.
- Weigh the client weekly; the client should gain no more than 3 lb/week.
- Progressively wean the client off of PN as prescribed to reduce the risk of metabolic problems, generally over 48 hours. If abruptly discontinuing a PN solution is necessary, replace it with 5% or 10% dextrose solution to prevent rebound hypoglycemia until the primary healthcare provider is notified and an intervention prescribed.
- Take steps to minimize the risk of infection.
- Dedicate only one port for PN and do not use the PN port to administer other solutions or medications.
- Ensure that the tubing has an in-line filter because of the high glucose level.
- Do not use a solution if a leak, cloudiness, or floating particles are identified.
- Apply and maintain a sterile transparent occlusive dressing over the insertion site.
- Use 70% alcohol pads or chlorhexidine gluconate-based pads to cleanse a port before and after use.
- Change parenteral infusion sets and fat emulsion sets every 24 hours.
- Change the dressing at least every 72 hours. Use meticulous sterile technique, wear a mask, and have the client not talk and turn the head away from the site when changing the dressing.
- Discard unused parenteral solution in 24 hours after its initiation.
- Document all nursing interventions and the client’s response.
C. Complications of parenteral nutrition and related nursing care
1. Pneumothorax: Air colleting in the pleural cavity precipitates collapse of the lung; owing to a puncture of the pulmonary system, generally during catheter insertion.
- Indicated by sudden severe chest pain, marked dyspnea, reduced oxygen saturation, and absent breath sounds on the side of the chest with the suspected pneumothorax.
- Elevate the HOB, administer oxygen, and monitor oxygen saturation.
- Assist with chest tube insertion if necessary to inflate the lung.
2. Catheter occlusion: Blockage of the lumen of the catheter; may be caused by a blood clot at the tip of the catheter.
- Indicated by a sluggish or an absent catheter flow rate.
- Stop the infusion.
- Attempt to relieve the obstruction following the prescription of the primary health-care provider or according to agency protocol.
- Flush the catheter with heparin or saline solution.
- If flushing is ineffective, attempt to aspirate the clot.
- If attempts to aspirate the clot are ineffective, follow agency protocol using a thrombolytic agent, such as urokinase.
3. Infection: Entrance of pathogenic microorganisms into the blood via the catheter or catheter insertion site.
- Indicated by elevated vital signs, chills, and positive blood culture.
- Administer prescribed antipyretics and local and/or systemic antibiotics.
4. Hyperglycemia and hypoglycemia: Increased blood glucose level (hyperglycemia)or decreased blood glucose level (hypoglycemia)due to an excessive or inadequate intake of glucose respectively.
- Hyperglycemia is indicated by polyuria, polydipsia, headache, and lethargy.
- Hypoglycemia is indicated by diaphoresis, shakiness, confusion, and loss of consciousness.
- Initiate and maintain a consistent flow rate as prescribed.
- Assess blood glucose level every 6 hours.
- Administer insulin according to the primary health-care provider’s prescription if the client experiences hyperglycemia.
- Administer glucose gel if the client experiences hypoglycemia.
D. Lipid emulsions and related nursing care
- Review the primary health-care provider’s history and physical for information indicating a history or presence of anemia; abnormal liver, biliary, or pancreatic function; or respiratory or coagulation impairments. Collaborate with the primary healthcare provider about these conditions because they are associated with fat emboli and the administration of parenteral lipids.
- Use a special administration set specific for lipids; use a new administration set for each bottle.
- Place the client in the supine position and have the client perform the Valsalva maneuver when connecting a catheter to the circulatory access to prevent an air embolus.
- Connect to the port below the filter if lipids are administered concurrently with PN because lipids will not pass through a PN filter because of their large particles.
- Ensure that the solution is free from froth and separation into layers.
- Ensure that lipids are at room temperature.
- Initially infuse 1 mL/min.
- Take the vital signs every 10 minutes for 30 minutes and assess for signs and symptoms of intolerance, indicted by fever, chills, flushing, nausea, vomiting, dyspnea, headache, and back pain.
- If no clinical indicators of intolerance occur, increase the flow rate to the prescribed rate and retake the vital signs every 4 hours.
- Complete the administration of lipids within 12 hours.
XII. MEDICATIONS ASSOCIATED WITH NUTRITION
When a person is diagnosed with a nutritional problem, the primary health-care provider can prescribe a variety of medications depending on the client’s need. The most common medications influencing a client’s nutritional status include antacids, antiemetics, anti-lipidemics, antisecretory agents, hypoglycemics, and insulin. Nurses should know the mechanisms of action, therapeutic and nontherapeutic effects, and nursing care related to these medications. This information is necessary not only to provide direct client care but also for client teaching because these medications are often self-administered over prolonged periods of time.
A. Antacids and related nursing care: Decrease gastric acidity, protect stomach mucosa, and reduce epigastric pain.
B. Antiemetics and related nursing care: Decrease nausea and vomiting; prevent and decrease motion sickness.
C. Anti-lipidemics and related nursing care: Decrease low-density lipoproteins (LDL),, triglycerides, and total cholesterol levels; increase high-density lipoproteins (HDL) levels.
D. Antisecretory agents and related nursing rare: Decrease gastric acidity and pain.
E. Oral hypoglycemics and related nursing care: Control blood glucose levels in type 2 diabetes.






