Sensory Disorders
Diagnostic Tests for the Eye
Fluorescein angiography a detailed imaging study used to assess problems with retinal circulation, such as those that occur in diabetic retinopathy, retinal bleeding, and macular degeneration, or to rule out intraocular tumors after administration of dye.
Pre-op Care:
- Assess the client for allergies to dye
- Obtain informed consent
- Administer mydriatic medication; instill into the eye 1 hour before the test
- The dye is injected into a vein of the client’s arm
- Inform the client about dye discomforts
- Inform client that the urine maybe bright green or orange for up to 2 days
- Observe for any untoward signs and symptoms
Post-Op Care:
- Encourage rest
- Increase OFI
- Remind the client that the yellow skin appearance will disappear
- Inform the client that the urine will appear bright green or orange until the dye is excreted
- Avoid direct sunlight for a few hours after the test; wear sunglasses, if staying outdoors
- Inform the client that the photophobia will continue until pupil size returns to normal
Computed tomography (CT) is performed to examine the eye, bony structures around the eye, and extraocular muscles; contrast maybe used if not contraindicated.
Interventions:
- No special client preparation or follow-up care needed
- Instruct the procedure to the client
- Ask about and document allergies
Slit lamp allows examination of the anterior ocular structures under microscopic magnification.
Interventions:
- Explain the procedure.
- Advise the client about the brightness of the light and the need to look forward at a point over the examiner’s ear.
Corneal staining a topical dye is instilled into the conjunctival sac to outline irregularities of the corneal surface that are not easily visible.
Interventions:
- Remove contact lenses
- Instruct to blink after the dye has been applied for proper distribution.
Tonometry the test is used primarily to assess for an increase in IOP and potential glaucoma.
- Noncontact tonometry: A puff of air is directed at the cornea to indent the cornea; less accurate method of measurement.
- Contact tonometry: A flattened cone is brought into contact with the cornea and the amount of pressure needed to flatten the cornea is measured; avoid rubbing the eye following the examination.
Note: Normal IOP is 10 to 21 mm Hg
Disorders of the Eye
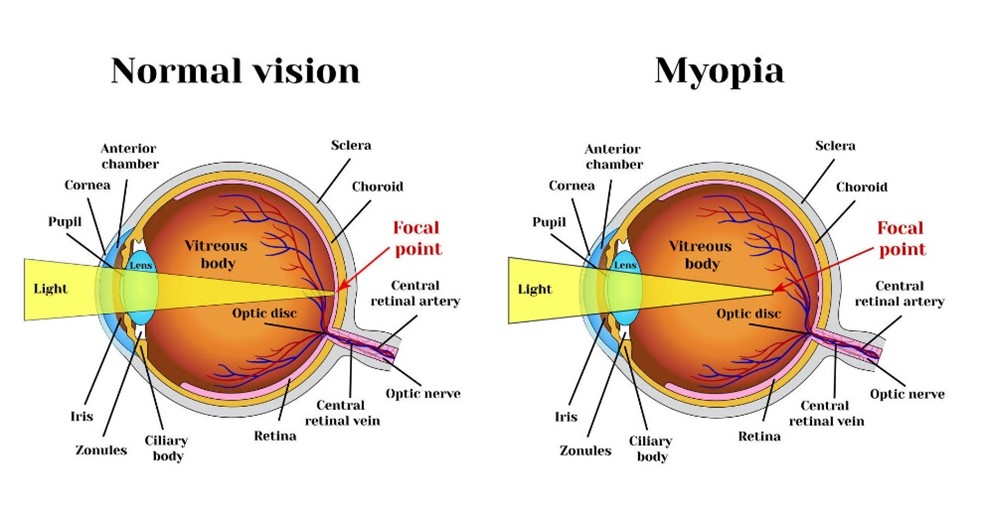
Refraction is the bending of light rays; any problem associated with eye length or refraction can lead to refractive errors.
Myopia (nearsightedness): Refractive ability of the eye is too strong for the eye length; images are bent and fall in front of, not on, the retina.
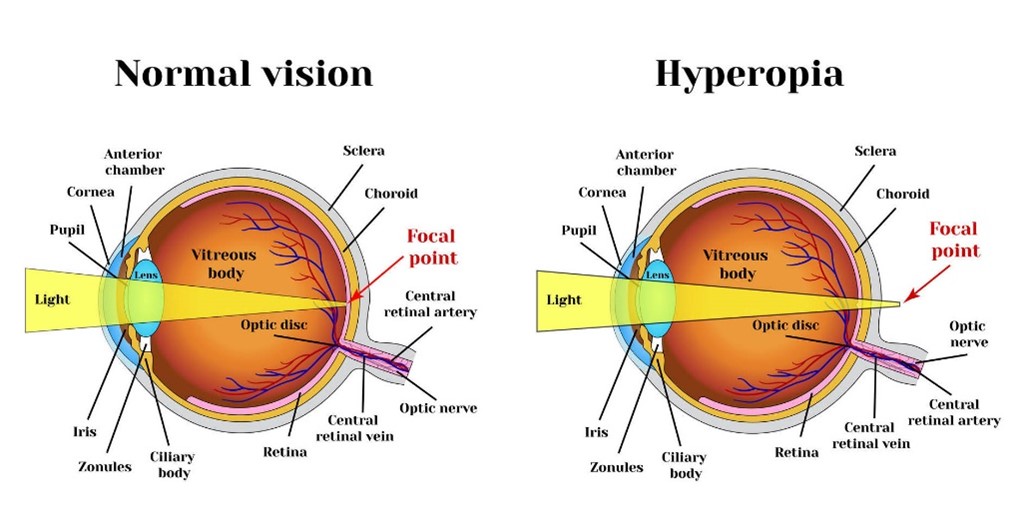
Hyperopia (farsightedness): Refractive ability of the eye is too weak; images are focused behind the retina.
Presbyopia: Loss of lens elasticity because of aging; less able to focus the eye for close work and images fall behind the retina.
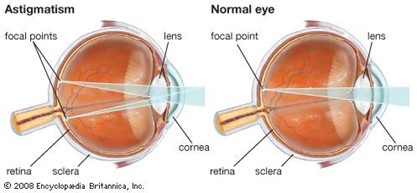
Astigmatism: Occurs because of the irregular curvature of the cornea; image focuses at 2 different points on the retina.
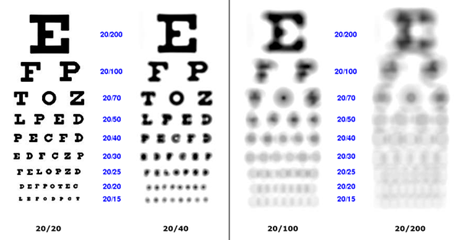
Legal blindness In the client who is legally blind, the best visual acuity with corrective lenses in the better eye is 20/200 or less, or the visual field is no greater than 20 degrees in its widest diameter in the better eye.
Nursing Interventions:
- Use a normal tone of voice when speaking to the client
- Alert the client when approaching
- Orient the client to the environment
- Ensure that the client has a clear pathway
- Promote independence
- * Allow the client to grasp the nurse’s arm at the elbow so that the client can detect the direction of movement.
- Instruct the client in the use of the cane for the blind (straight shape, white color with red tip)
Cataract is "opacity of the lens" that distorts the image projected onto the retina and that can progress to blindness.
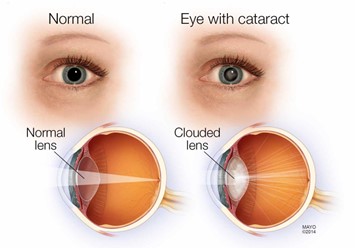
Signs and Symptoms:
- Early signs: Blurred vision and decreased color perception
- Late signs: Diplopia,reduced visual acuity, absence of the red reflex, and the presence of a white pupil
- Pain or eye redness is associated with age-related cataract formation.
- Loss of vision is gradual
Pre-op Care:
- Instruct the importance of hand washing and measures to prevent or decrease IOP (bending over, coughing, straining, and rubbing the eye)
- Administer eye medications preoperatively, including mydriatics and cycloplegics as prescribed.
Post-op Care:
- Elevate the head o the bed 30 to 45 degrees
- Turn the client to the back or nonoperative side
- Maintain an eye patch as prescribed; orient the client to the environment
- Position the client’s personal belongings to the nonoperative side
- Use side rails for safety
- Assist with ambulation
- Protective glasses must be worn at all times
- Eye itching and mild discomfort are normal for a few days after the procedure.
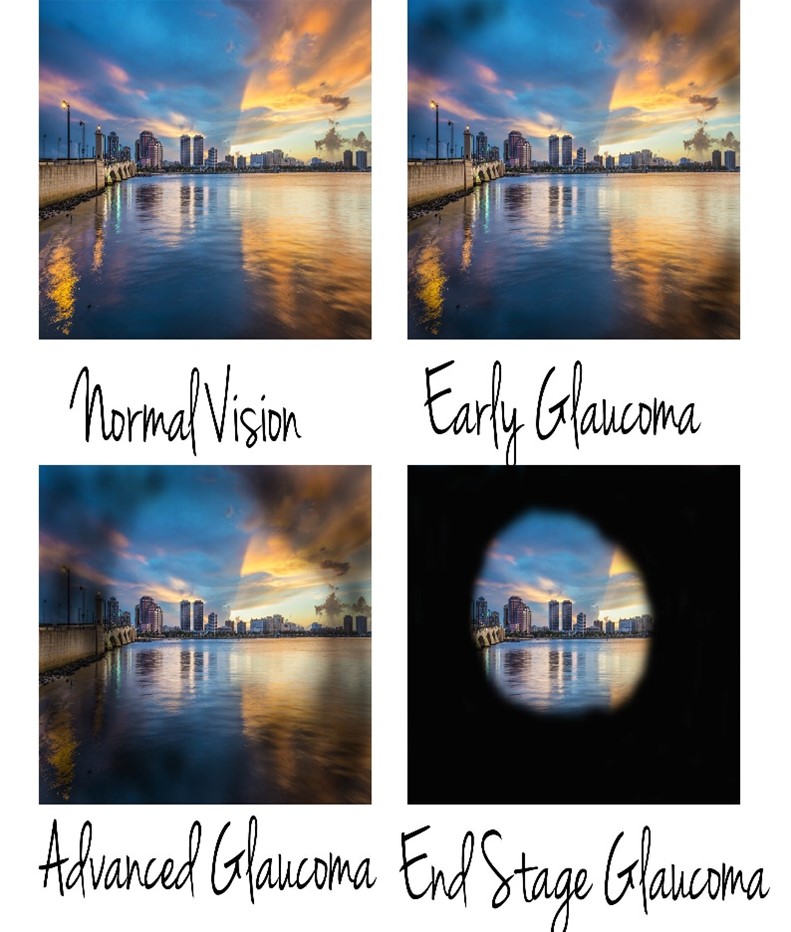
Glaucoma the condition damages the optic nerve and can result in blindness due to IOP. "Tunneling of visual fields"
Types:
- Primary open-angle glaucoma (POAG): results from obstruction to out flow of aqueous humor and is the most common type
- Primary angle-closure glaucoma (PACG) results from blocking the outflow of aqueous humor into the trabecular mesh work
Vision:
Retinal detachment detachment or separation of the retina from the epithelium; can lead to blindness. "Curtain-like vision"
Signs and Symptoms:
- Flashes of light
- Floaters or black spots (signs of bleeding)
- Increase in blurred vision
- Sense of a curtain being drawn over the eye
- Loss of a portion of the visual field; painless loss of central or peripheral vision
Nursing Interventions:
- Provide bed rest
- Cover both eyes with patches to prevent further detachment
- Speak to the client before approaching
- Protect the client from injury
- Draining fluid from the subretinal space so that the retina can return to the normal position.
- Diathermy, the use of an electrode needle and heat through the sclera, to stimulate an inflammatory response
- Laser therapy, to stimulate an inflammatory response and seal small retinal tears before the detachment occurs
- Scleral buckling, to hold the choroid and retina together with a splint until scar tissue forms, closing the tear
- Insertion of gas or silicone oil to promote reattachment; these agents float against the retina to hold it in place until healing occurs.
- Maintain eye patches
- Monitor for hemorrhage
- Prevent nausea and vomiting and monitor for restlessness, which can cause hemorrhage.
- Instruct the client to limit reading for 3 to 5 weeks
Macular Degeneration caused by gradual blocking of retinal capillaries leading to an ischemic and necrotic macula; rod and cone photo receptors die.
Vision:

Signs and Symptoms:
- A decline in central vision
- Blurred vision and distortion
Nursing Interventions:
- Initiate strategies to assist in maximizing remaining vision
- Promote independence.
- Laser therapy, photodynamic therapy may be prescribed to seal the leaking blood vessels in or near the macula
Ocular Melanoma most common malignant eye tumor in adults; found in the uvealt ract and can spread easily.
Signs and Symptoms:
- Increased IOP
- Blurring of vision
- Change of iris color
Nursing Interventions:
- Enucleation (surgical removal of the eye)
- Radiation therapy
Foreign bodies an object such as dust or dirt that enters the eye and causes irritation.
Nursing Interventions:
Visible object: Look upward > Expose the lower lid > Wet a cotton-tipped applicator (NSS) > Twist the swab over the particle > Remove it.
Not visible object: Look downward > Place a cotton applicator horizontally on the outer surface of the upper eye lid > Grasp the lashes > Pull the upper lid outward > Remove it.
Penetrating objects an eye injury in which an object penetrates the eye.
Nursing Interventions:
- Never remove the object
- Cover the eye with a cup (paper or plastic) and tape in place
- Do not bend over or lie flat or place pressure on the eye
- X-rays and CT scans of the orbit are usually obtained.
- NO MRI
Chemical burns an eye injury in which a caustic substance enters the eye.
PRIORITY NURSING ACTIONS!
- Quickly assess the client and visual acuity.
- Check the pH of the eye (pH: 7.35 - 7.45)
- Irrigate the eye using lactated ringers solution (15-20 minutes)
- Document the event, actions taken, and the client’s response
Disorders of the Ear
Diagnostic Tests for the Ear
Tomography assesses the mastoid, middle ear, and inner ear structures and is especially helpful in the diagnosis of acoustic tumors.
Nursing Interventions:
- All jewelry is removed.
- Lead eye shields are used to cover the cornea against radiation
- Remain still in a supine position
- No follow-up care is required.
- If contrast is to be used, assess for any allergies
Audiometry measures hearing acuity
- Pure tone audiometry is used to identify problems with hearing, speech, music, and other sounds in the environment.
- Speech audiometry, the client’s ability to hear spoken words is measured.
Electronystagmography (ENG) is used to distinguish between normal nystagmus and medication-induced nystagmus, or nystagmus caused by a lesion in the central or peripheral vestibular pathway.
Nursing Interventions:
- Instruct to remain NPO for 3 hours before testing
- Avoid caffeine-containing beverages for 24 to 48 hours before the test.
- Medications are withheld for 24 hours before testing
- Instruct the client that this is a long and tiring procedure.
- Bring prescription eyeglasses to the examination
- The client’s ears are irrigated with cool and warm water, causes nausea and vomiting.
- Assist with ambulation
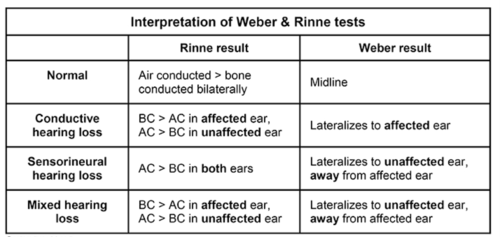
Conductive hearing loss occurs when sound waves are blocked to the inner ear fibers because of external or middle ear disorders
Sensorineural hearing loss is often permanent, and measures must be taken to reduce further damage.
Mixed hearing loss also known as conductive-sensorineural hearing loss. The client has both sensorineural and conductive hearing loss.
Signs of Hearing Loss
- Frequently asking others to repeat statements
- Straining to hear
- Turning the head or leaning forward to favor 1 ear
- Shouting in conversation
- Ringing in the ears
- Failing to respond when not looking in the direction of the sound
- Answering questions incorrectly
- Raising the volume of the television or radio
- Avoiding large groups
- Better understanding of speech when in small groups
- Withdrawing from social interactions
Cochlear implantation used for sensorineural hearing loss; small computer converts sound waves into electrical impulses; Electrodes are placed by the internal ear with a computer device attached to the external ear.
Presbycusis leads to degeneration or atrophy of the ganglion cells in the cochlea and a loss of elasticity of the basilar membranes.
External otitis infective inflammatory or allergic response involving the structure of the external auditory canal or auricles; common in children.
Signs and Symptoms:
- Pain
- Itching
- Plugged feeling in the ear
- Redness and edema
- Exudate
- Hearing loss
Nursing Interventions:
- Apply heat locally for 20 minutes, 3 times a day.
- Encourage rest to assist in reducing pain.
- Administer antibiotics or corticosteroids as prescribed.
- Administer analgesics for the pain as prescribed.
- Keep the affected ear clean and dry.
- Use earplugs for swimming.
- Avoid the use of hair products or headphones
Mastoiditis results from untreated or inadequately treated chronic or acute otitis media.
Signs and Symptoms:
- Swelling behind the ear and pain with minimal movement of the head
- Cellulitis on the skin or external scalp over the mastoid process
- A reddened, dull, thick, immobile tympanic membrane
- Low-grade fever
- Tender and enlarged post auricular lymph nodes
Nursing Interventions:
- Most common treatment: Simple or modified radical mastoidectomy with tympanoplasty
- Once infected tissue is removed, the tympanoplasty is performed to restore normal hearing.
Otosclerosis a genetic disorder of the labyrinthine capsule of the middle ear that results in a bony overgrowth of the tissue surrounding the ossicles.
Signs and Symptoms:
- Slowly progressing conductive hearing loss
- Bilateral hearing loss
- A ringing or roaring type of constant tinnitus
- Loud sounds heard in the ear when chewing
- Pinkish discoloration (Schwartze’s sign) of the tympanic membrane
- Negative Rinne test
- Weber’s test shows lateralization of sound to the ear with the greatest degree of conductive hearing loss
Fenestration is the removal of the stapes, with a small hole drilled in the footplate; a prosthesis is connected between the incus and footplate.
Pre-op Care:
- Prevent middle ear or external ear infections.
- Instruct the client to avoid excessive nose blowing.
Post-op Care:
- Inform that Gel foam ear packing (if used) may interferes with hearing to decrease bleeding.
- Assist with ambulating during the first 1 to 2 days after surgery.
- No noticeable improvement in hearing may occur for as long as 6 weeks.
- Administer antibiotic, ant vertiginous, and pain medications as prescribed.
- Instruct the client to move the head slowly when changing positions
- Instruct the client to avoid rapid extreme changes in pressure (quick head movements, sneezing, nose blowing, straining, and changes in altitude)
Labyrinthitis infection of the labyrinth that occurs as a complication of acute or chronic otitis media.
Signs and Symptoms:
- Hearing loss on the affected side
- Tinnitus
- Spontaneous nystagmus (affected side)
- Vertigo
- Nausea and vomiting
Nursing Interventions:
- Monitor for signs of meningitis most common complication, (headache, stiff neck, lethargy)
- Advise the client to rest in bed in a darkened room.
- Administer antiemetics and ant vertiginous medications as prescribed
Meniere’s Syndrome also called endolymphatic hydrops; it refers to dilation of the endolymphatic system by overproduction or decreased reabsorption of endolymphatic fluid.
Signs and Symptoms:
- Tinnitus
- Unilateral sensorineural hearing loss
- Vertigo
- Feelings of fullness in the ear
- Nausea and vomiting
- Severe headaches
Nonsurgical interventions:
- Prevent injury (SAFETY)
- Provide bed rest in a quiet environment.
- Aid with walking.
- Instruct the client to move the head slowly
- Initiate sodium and fluid restrictions
- Instruct the client to avoid watching television (during acute attack)
- Administer nicotinic acid, antihistamine, antiemetics as prescribed
Surgical interventions:
- Endolymphatic drainage and insertion of a shunt
- Labyrinthectomy
Post-op Care:
- Assess packing and dressing on the ear.
- Speak to the client on the side of the unaffected ear.
- Maintain safety.
- Assist with ambulating
- Administer ant vertiginous and antiemetic medications as prescribed.
Works Cited






